Brain Tumour
A brain tumour is a growth of cells in the brain that multiplies in an abnormal, uncontrollable way.
Grades and Types of Brain Tumour
Brain tumours are graded according to how fast they grow and how likely they are to grow back after treatment.
Grade 1 and 2 tumours are low grade, and grade 3 and 4 tumours are high grade.
There are 2 main types of brain tumours:
- Non- cancerous (benign) brain tumour
- Cancerous (malignant) brain tumour
Non-Cancerous ( BENIGN ) Brain Tumours:
– these are low grade (grade 1 or 2), which means they grow slowly and are less likely to return after treatment
Cancerous ( MALIGNANT) Brain Tumours
– these are high grade (grade 3 or 4) and either start in the brain (primary tumours) or spread into the brain from elsewhere (secondary tumours); they're more likely to grow back after treatment.
Symptoms of a Brain Tumour
The symptoms of a brain tumour vary depending on the exact part of the brain affected.
Common Symptoms include:
- headaches
- seizures (fits)
- persistently feeling sick (nausea), being sick (vomiting) and drowsiness
- mental or behavioural changes, such as memory problems or changes in personality
- progressive weakness or paralysis on one side of the body
- vision or speech problems
- Sometimes you may not have any symptoms to begin with, or they may develop very slowly over time.
Benign Brain Tumour (non-cancerous)
A benign (non-cancerous) brain tumour is a mass of cells that grows relatively slowly in the brain. Non-cancerous brain tumours tend to stay in one place and do not spread. It will not usually come back if all of the tumour can be safely removed during surgery.
If the tumour cannot be completely removed, there's a risk it could grow back. In this case it'll be closely monitored using scans or treated with radiotherapy.
Types and grades of non-cancerous brain tumour
There are many different types of non-cancerous brain tumours, which are related to the type of brain cells affected.
Examples include:
- gliomas – tumours of the glial tissue, which hold and support nerve cells and fibres
- meningiomas – tumours of the membranes that cover the brain
- acoustic neuromas – tumours of the acoustic nerve (also known as vestibular schwannomas)
- craniopharyngiomas – tumours near the base of the brain that are most often diagnosed in children, teenagers and young adults
- haemangioblastomas – tumours of the brain's blood vessels
- pituitary adenomas – tumours of the pituitary gland, a pea-sized gland on the under surface of the brain
Brain tumours are graded from 1 to 4 according to how fast they grow and spread, and how likely they are to grow back after treatment.
Non-cancerous brain tumours are grades 1 or 2 because they tend to be slow growing and unlikely to spread.
The not cancerous brain tumour can often be successfully treated, but they're still serious and can be life threatening.
Symptoms of non-cancerous brain tumours
The symptoms of a non-cancerous brain tumour depend on how big it is and where it is in the brain. Some slow-growing tumours may not cause any symptoms at first.
Common symptoms include:
- new, persistent headaches
- seizures (epileptic fits)
- feeling sick all the time, being sick, and drowsiness
- mental or behavioural changes, such as changes in personality
- weakness or paralysis, vision problems, or speech problems
Malignant Brain Tumour (brain cancer)
A malignant brain tumour is a cancerous growth in the brain. It's different from a benign brain tumour, which isn't cancerous and tends to grow more slowly.
Symptoms
The symptoms of a brain tumour depend on where it is in the brain.
Common symptoms include:
- headaches (often worse in the morning and when coughing or straining)
- fits (seizures)
- regularly feeling sick (vomiting)
- memory problems or changes in personality
- weakness, vision problems or speech problems that get worse
- See a GP if you have symptoms of a brain tumour that don't go away. It's unlikely to be a tumour, but it's best to be sure.
Types
There are lots of types of brain tumour. They have different names depending on where they are in the brain. They're also given a number from 1 to 4, known as the grade.
The higher the number, the more serious a tumour is:
- grade 1 and 2 brain tumours are non-cancerous (benign) tumours that tend to grow quite slowly
- grade 3 and 4 brain tumours are cancerous (malignant) tumours that grow more quickly and are more difficult to treat
Brain tumours are also called primary (which start in the brain) and secondary (which spread to the brain).
Treatments
Treatment for a brain tumour aims to remove as much of it as possible and try to stop it coming back.
The main treatments are:
- surgery – a small section of skull is removed and the tumour is cut out before the piece of skull is fixed back in place
- radiotherapy – radiation from an external machine is used to kill cancer cells after surgery
- chemotherapy – medicine is used to kill cancer cells after surgery, or relieve symptoms if the tumour can't be removed
- radiosurgery – lots of tiny beams of radiation are aimed at the cancer to kill it if you can't have surgery
- carmustine implants (glial wafers) – a new way of giving chemotherapy for some high-grade tumours, where implants are inserted into the brain
- Medicines may also be used to relieve symptoms like headaches, seizures and being sick (vomiting).
Outlook
The outlook for a malignant brain tumour depends on things like where it is in the brain, its size, and what grade it is. It can sometimes be cured if caught early on, but a brain tumour often comes back and sometimes it isn't possible to remove it.
Recovery and after effects
After treatment, you might have some lasting problems, such as:
- seizures
- walking difficulties
- speech problems
You may need treatment and support like occupational therapy and physiotherapy to help you recover or adapt to any problems.
It's important to follow a healthy lifestyle to lower your risk of stroke. This means stopping smoking if you smoke, following a healthy diet and doing regular exercise.
You may be able to gradually return to your normal activities as you recover, although some things (like contact sports) may need to be avoided for life.
Side effects of treatment
Some people who have had a brain tumour can develop side effects from treatment months or years later, such as:
- cataracts
- epilepsy
- problems with thinking, memory, language or judgement
- very rarely stroke can happen.
BRAIN CANCER DATA Period 2020 -2025
Hospital Trials and Treatment with our NEW medications & Innovative methods
BRAIN CANCER DATA Period 2020-2025
Mortality in EU 2020-2025:
386,811 (After Standard EU hospital Treatment being used only)
Mortality in the UK 2020-2025:
32,496 (After Standard UK hospital Treatment being used only)
RESULT by OUR NEW METHODS (Used from 2014-2019) and by
OUR NEW INNOVATIVE METHODS (Used from 2020-2025+)
Testing Period 2020-2025; All Age Groups, Tested patients in the UK, Switzerland, Germany and Italy:
Total individuals/patients involved: 210,252 (100%) of which:
- Fully recovered patients: 20.4%
- Recovered (No treatment needed for the period of 2 years, monitoring every 6 months: 24.5%
- Partially Recovered (Further treatment needed as precautionary after 3-6 months passed): 38.8%
- Unknown Recovery/Non-Recovery Data available: 15.7%
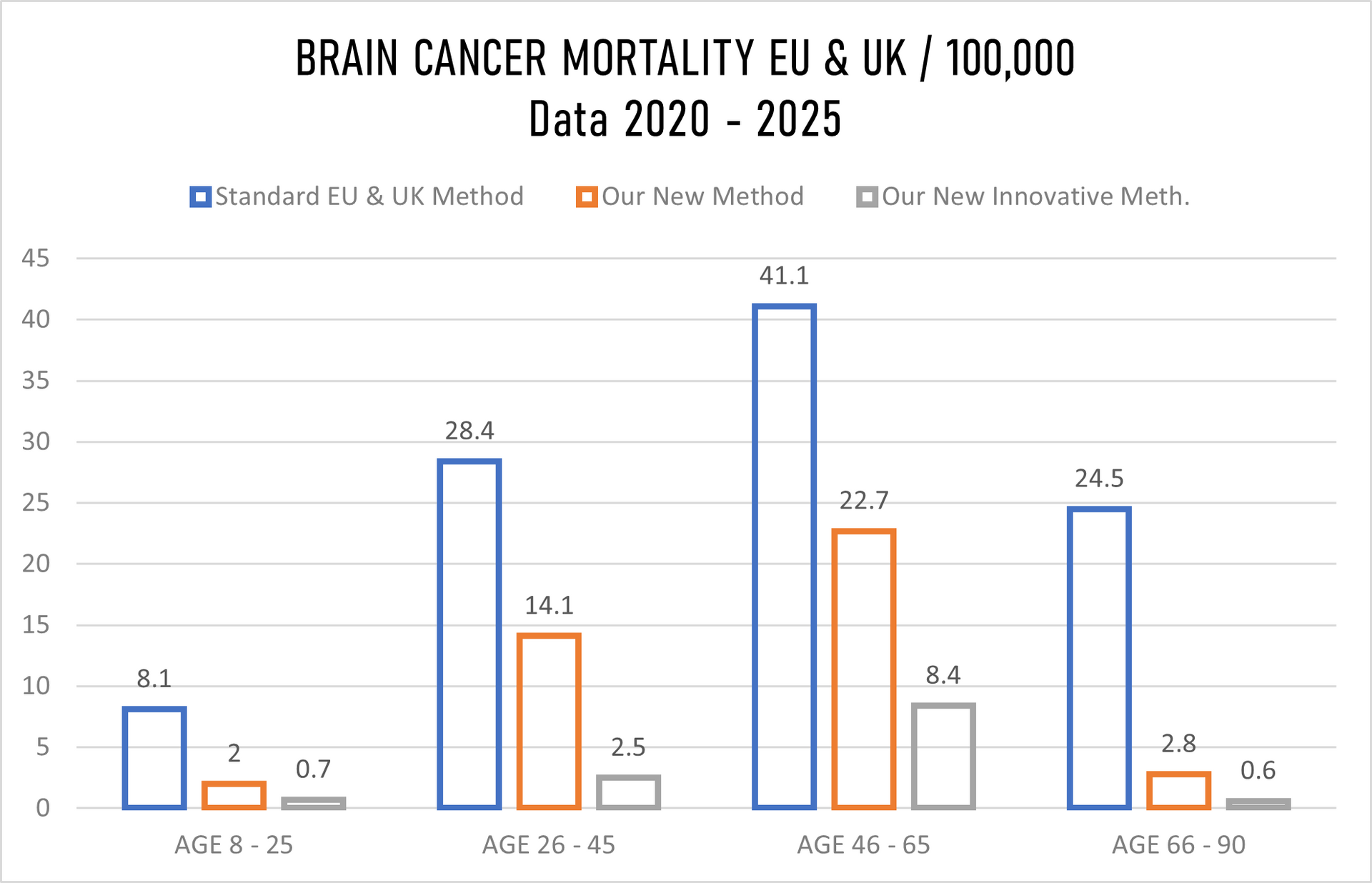
- Deaths in Total: 0.6% (The highest % with the group 46-65).
Topics used in our research described along with MCCD's:
01. Tumour cell biology, heterogeneity and plasticity
02. Microenvironment
03. Imaging
04. Computational neuro-oncology
05. Advanced diagnostics and biomarkers
06. Neurocognition and connectome
07. Neurosurgery, drug delivery and advanced techniques
08. Immunotherapy
09. Radiation
10. Pediatric brain tumors
11. Brain metastasis and leptomeningeal disease
12. Adult glioma
13. Meningioma
14. Rare CNS tumors
15. Palliative and supportive care/QoL
16. Public cancer policies and patient involvement
17. Clinical neuro-oncology
18. Preclinical neuro-oncology
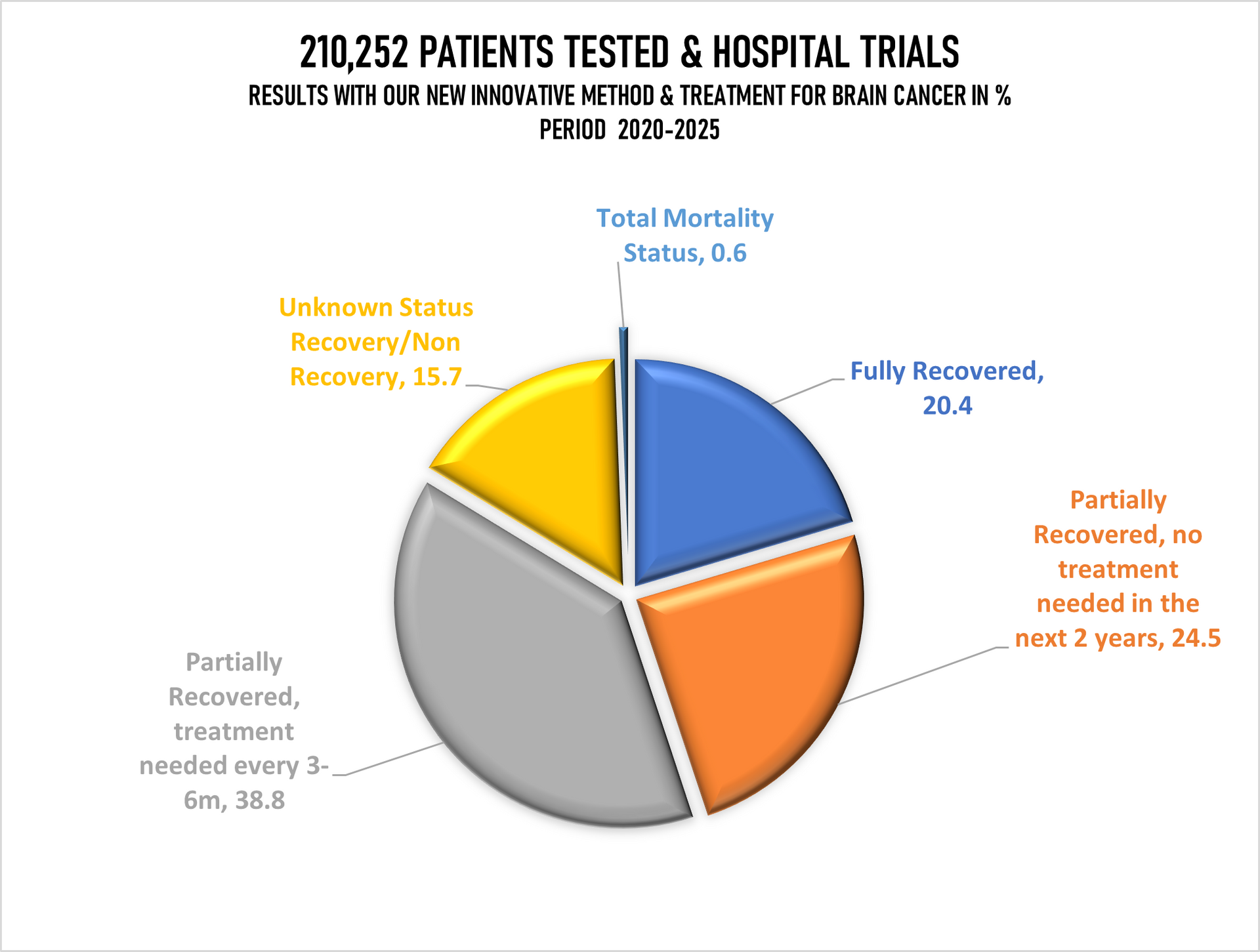
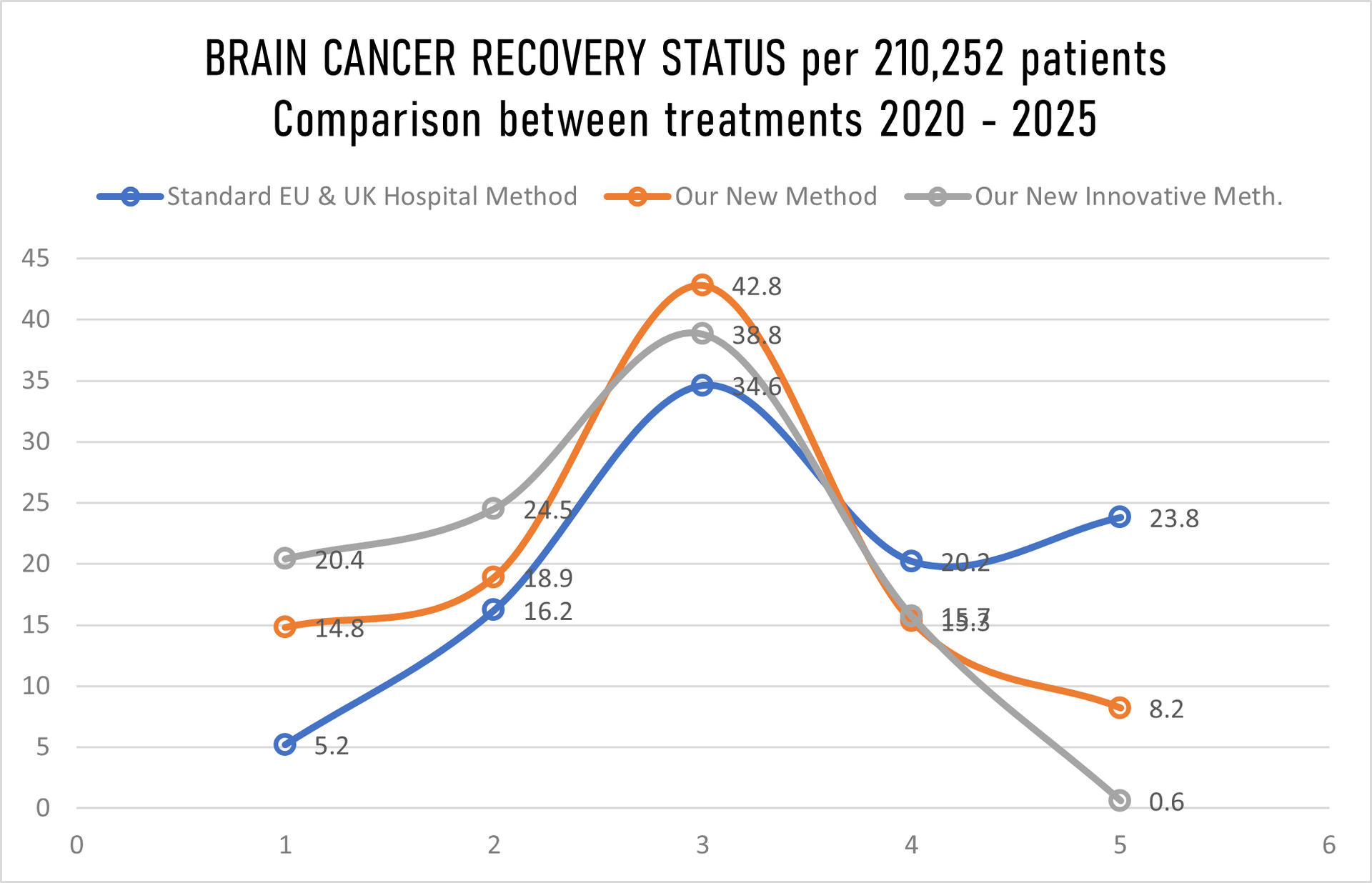
The graph above showing recovery/non-recovery status on 210,252 patients randomly taken for hospital trials and treatment where we have in
Stage 1 just 10% patients, Stage II just 20%, Stage III 30% and in Stage IV staggering 40% patients while hospitals in EU & UK gave us details for the same number of patients (210,252) in Stage 1 40%, Stage II 30%, Stage 3 20% and in Stage IV only10%. That further means that we have our mortality rate with innovative treatment well above all expectation low, sadly still 1(one) patients passed away despite that we overtake 40% of 210,252 patients with Stage IV cancer, in meanwhile under the standard hospital treatment in EU & UK 50 patients past away, having in mind that they have in Stage IV just 10% patients while we have 40%.
| Number of patients of 210,252 | Cancer Stage I | Cancer Stage II | Cancer Stage III | Cancer Stage IV |
|---|---|---|---|---|
| By Standard treatment in EU & UK hospital | 84,100 | 63,075 | 42,050 | 21,077 |
| By Our New Medications | 21,077 | 42,050 | 63,075 | 84,100 |
| By Our Innovative treatment | 21,077 | 42,050 | 63,075 | 84,100 |
REFERENCES TO THE DATA ABOVE (Period 2020-2025):
AGE GAP:
The youngest person was 8 years 3 months and 17 days of age
The oldest person was 90 years 1 month and 5 days of age
GENDER:
Female: 89,112 of 210,252
Male: 121,140 of 210,252
Age group 8-25 > 4.4%
Age group 26-45 > 28.6%
Age group 46-65 > 45.7%
Age group 66-90 > 21.3%
--------------------------------
Total: 100%
=======================
METHODS COMPARISONS:
- Old Methods meaning the STANDARD METHODS used by the general hospitals on a daily basis for the last minimum 5 years in Europe and in the United Kingdom.
- Our Methods meaning our NEW MEDICATION/TREATMENT with which we came out after over 14 years of research and tests.
- Our Innovative Methods Combine meaning our NEW INNOVATIVE MEDICATION & TREATMENT COMBINED in crossed double parallel treatment > NEW INNOVATIVE MEDICATION and different way of treatment combined with chemotherapy or combined with radiotherapy or combined with chemo and radiotherapy both together.
Separately we tested our under #2 above and #3 above combined with "OLD " methods used by the majority hospitals in Europe and in the United Kingdom however, the final readings cannot be 100 percent accurate and cannot be as such used for whatever comparison as the data across the United Kingdom and Europe are not 100 percent accurate.
MORTALITY:
In the Europe 2020-2025 > 16.3% (Going Up). In the United Kingdom 2020-2025 > 12.9% (Going Up)
With our NEW Innovative Treatment and Medication in Europe & United Kingdom 2020-2025 less that 1% (Just 0.6%) mortality rate was recorded.
The % of "Unknown Recovery / Non-Recovery" went up: 2018/23 was 15%, and 2019/2024 was to 16.1% mainly in both periods at the same age group 32-44 which we believe has increased due to usage of control drugs or drugs, heavily drinking and smoking. This group is now monitored separately for the second time.
There is an increase of mortality in Europe for 1.4% while in the UK mortality went up by 1.8%, yet again not hundred percent accurate data as hospitals around Europe and United Kingdom "escape" registration of the death to "push" death patient to different group as of course of the death.
All patients being chosen randomly what also might be the point of under 1% mortality rate.
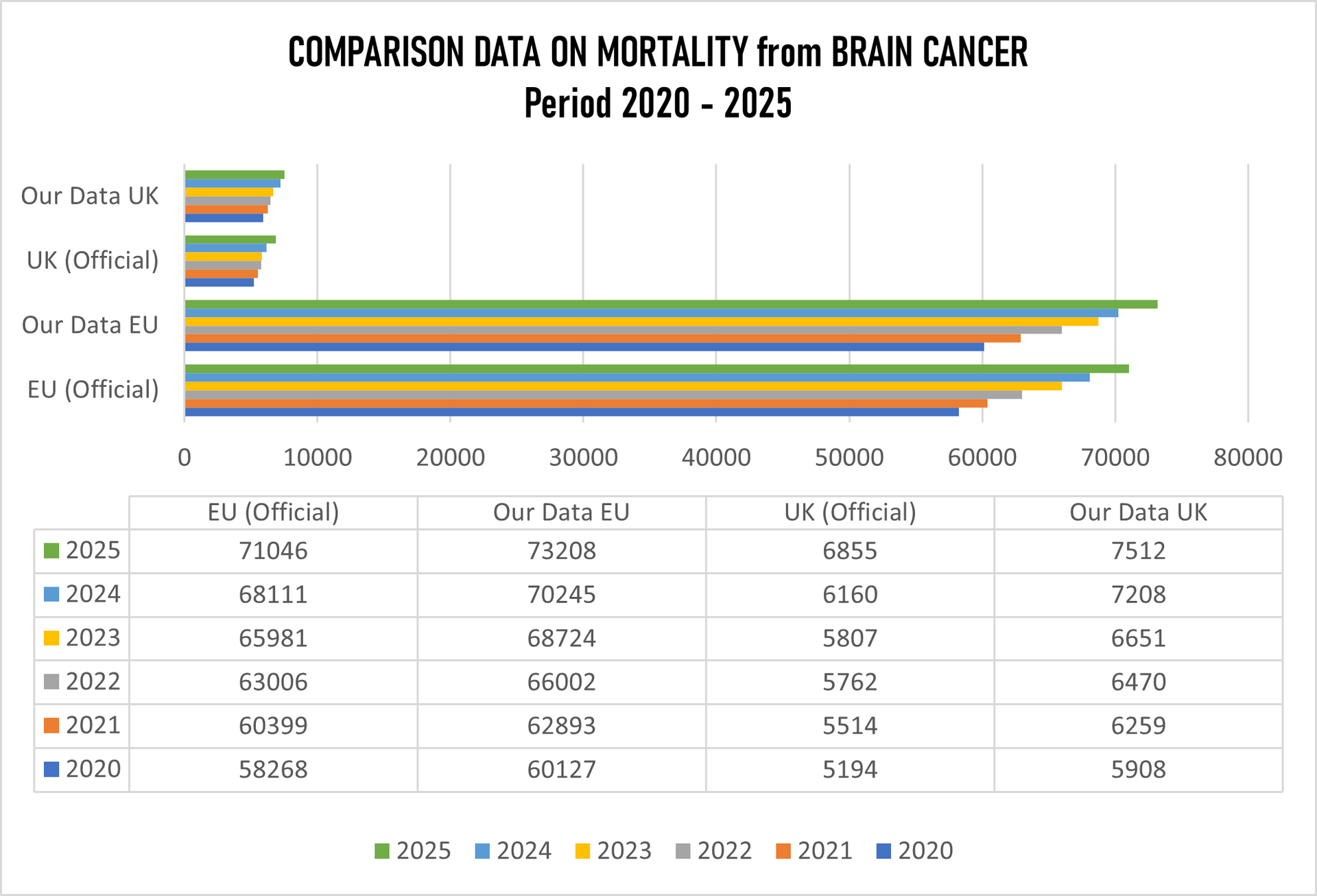
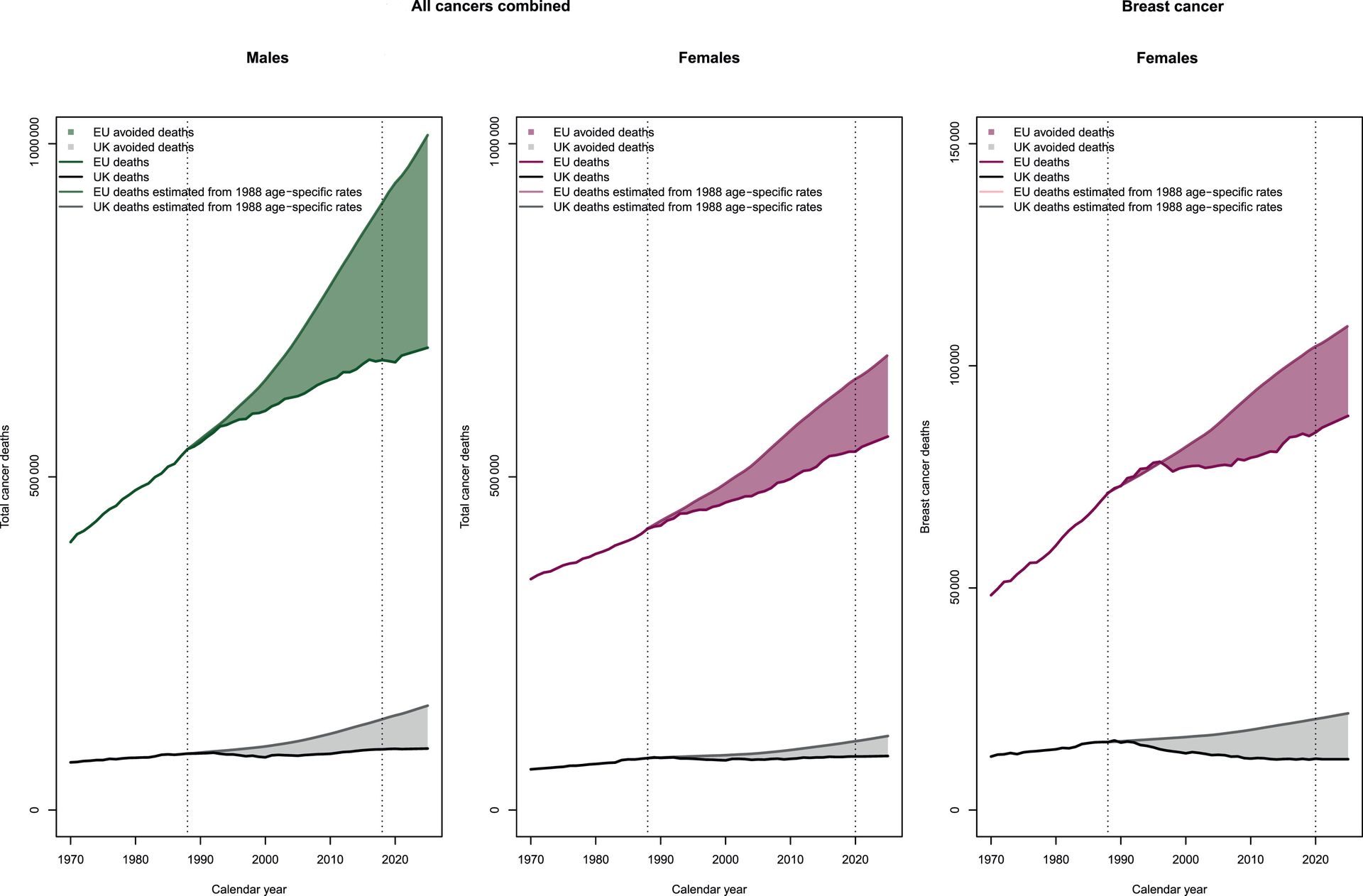
From the table above it is clearly seen that the figures are very much different. The so-called "official" data are not accurate when deaths from brain cancer are concerned which include deaths also on other nervous system (CNS), not in Europe, even less in the United Kingdom.
Europe claims "official" data on mortality from brain cancer is 386,811 deaths, while by our data the figure for Europe (without United Kingdom) is 401,199 which presents 14,388 deaths more.
The UK "official" data are 35,292 deaths, while our number for the same period is 40,008 which is 4,716 more deaths from official data.
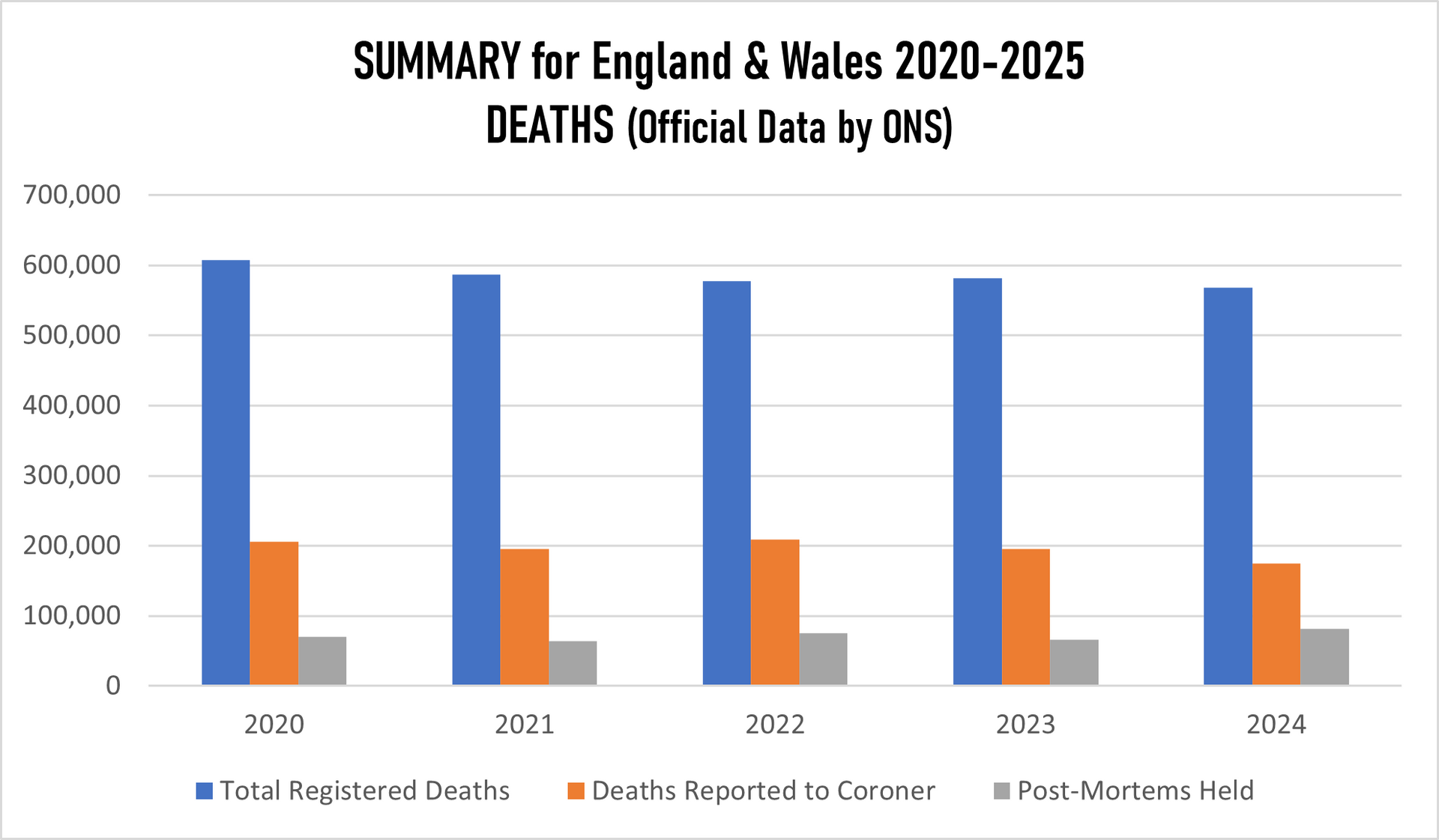
We tried to figure out how the "official" report was put together where the Office for the National Statistics (ONS) is the primary source for mortality statistics in England and Wales, using data from death certificates to identify breast cancer as the underlying cause. Therefore the basics is Medical Certificate of Death (MCCD). In England in Wales the Medical Examiner Scrutiny is used (since 2024), which is statutory Medical Examiner (ME). However if the death was unexpected or sudden or the cause is unknown the coroner gets involved who might or not order a post-mortem. Yet again, the number of post-mortem examinations for breast cancer deaths is extremely low because they considered breast cancer as "natural cause" and the number of inquest and by extension has been significantly decreasing.
While there were significant improvements made with treatment of the "classic" brain tumour which normally everywhere are dealt with surgery, chemotherapy and radiotherapy there is still complete "darkness" how to deal with glioblastoma.
UK "official" statistics showing that the numbers have reached the lowest level on a record that is not entirely correct because figures are well up in comparison with the year before. Even more dramatic is that the "official" data are showing that brain cancer remains the biggest killer of childrens and young adults up to age 40.
We have to be aware that there are more than 100 different types of brain tumours. This is a huge and diverse set of tumours, where some of which are incredibly rare and many medical professionals have not even heard about them. Therefore, analysis can vary significantly between institutions and reporting organisations and may change with new scientific discoveries. These groupings can also sometimes lack the detail needed to reflect actual patient experiences. So, when we see “brain tumour” in a dataset, it might mean very different things depending on where it came from.
The term “brain tumour” is also used more broadly to include tumours in other parts of the central nervous system, such as the spinal cord, meninges and cranial nerves. Terms like “brain cancer” and “brain tumour” may seem interchangeable, but they hold distinct definitions for clinicians and researchers, which are therefore important to understand. The term “brain tumour” covers both cancerous and non-cancerous tumours. So, it is essential that statistics clearly indicate whether they refer to brain tumours or brain cancer.
We have to understand the difference between primary and secondary brain tumours.
Primary brain tumours start in the brain itself, while secondary (or metastatic) brain tumours begin elsewhere in the body and spread to the brain. This distinction matters because they often behave differently, require different treatments and are tracked separately in data systems. All these data whether it is going for primary or secondary brain tumours is not seen by any so-called "official data" not in the United Kingdom not in Europe.
Why that would be important? Knowing all the above there should be meaningful comparison across organisations, regions and time periods to spot trends and disparities in care and outcomes which simply does not happen. Research centres and other similar institutions are keeping their data as "top secret" therefore, there is minor or no collaboration between centres where knowledge and support should be the primary target - sharing the data and exchange the data about treatments and survival rates
It is fact that each person is unique, and their individual journey is not necessarily represented by the general figures and averages provided by statistics.
OUR RESEARCH and MORTALITY DATABASE 2020-2025
Cancer is one of the biggest health challenges worldwide. Since starting the research in 2011/12, the percentage of all deaths from cancer has risen from 9.6% in 2011 to 14.9% 10 years later; in the last 5 years this has risen again to where we now have 16.8% on top of the previous five years screening of all deaths recorded as cancer deaths.
Taking into consideration that in the period 2020-2025 the average European and the United Kingdom population was 762.7 million, an average 5,128,206 new cases were reported during the same period. This is an ASR of 282, and a cumulative risk of 31.28%.
Breast, Colorectum, and Lung cancers were the most common cancers across both sexes.
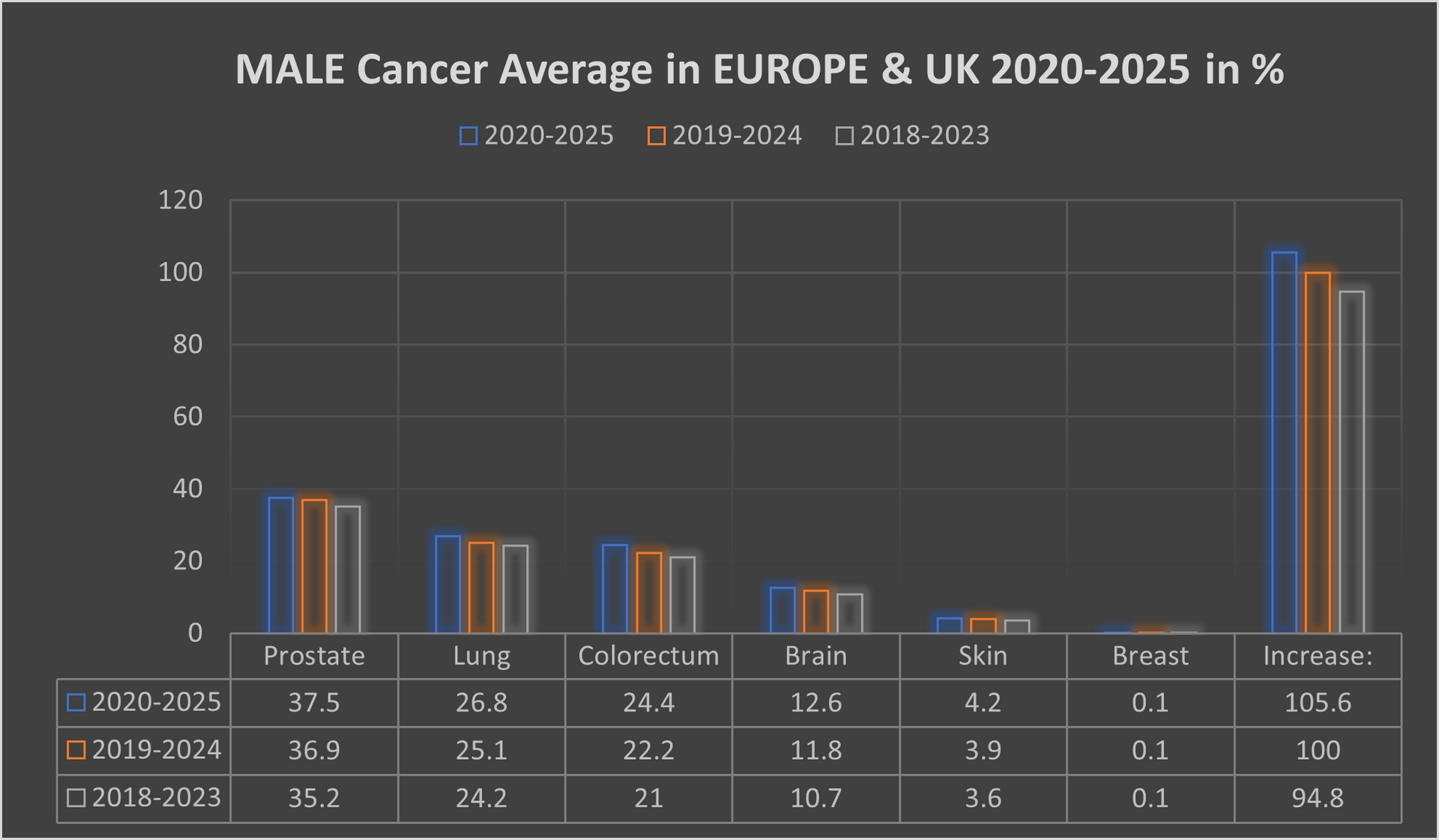
The male population in this period, some 271.4 million, recorded an average of 2,617,448 new cancer cases per year; an ASR of 32.7% per 100,000 and a cumulative risk of 34.6%.
The top 3 most common cancers among males were Prostate, Lung, and Colorectum cancer.
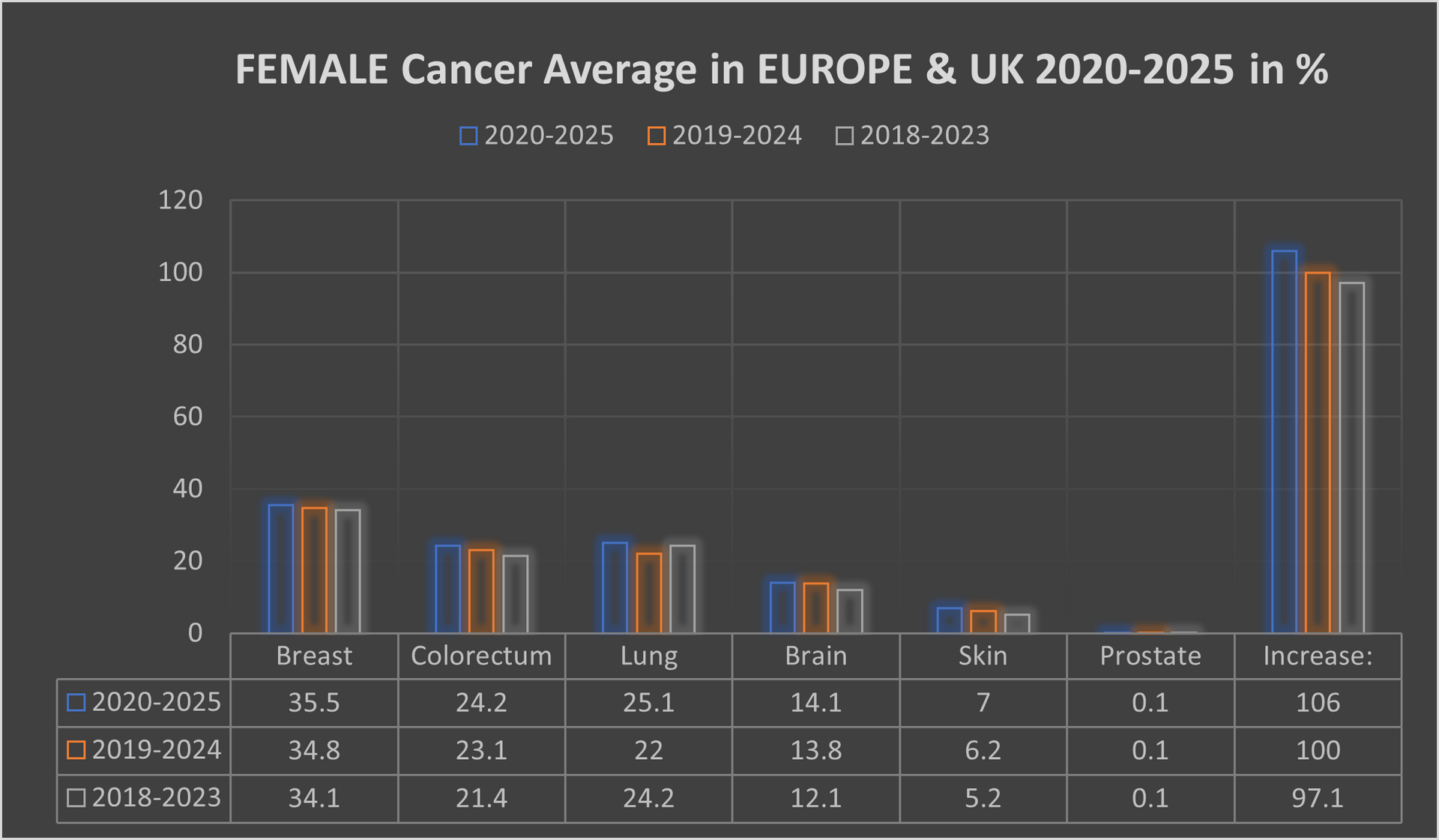
The female population in this period, some 291.3 million, recorded an average 2,494,488 new cancer cases per year; an ASR of 26.8% and a cumulative risk of 27.5%.
The top 3 most common cancers in females were Breast, Colorectum, and Lung cancer.
A significant point with cancer in the female population was switching lung cancer from 3rd place to 2nd place, with colorectum cancer dropped back from 2nd place to 3rd place.
Our mortality database is a collection of death registration data which includes cause of death information from member states; we use only the data which has been properly coded to the International Classification of Diseases (ICD).
What has also changed in recent years is the age of the death rate. This had declined over time in several countries due to life improvements, early diagnoses, medical advances, and a general reduction in risk factors like smoking and even drinking. However, there is a worrying emerging trend with rates of cancer in the population group aged up to 16.
This is rising well over expectations, especially in the United Kingdom, Spain, France and lately also in Italy.
IMPORTANT: If you are interested on details by countries, areas, hospitals we can provide all the details which include also data over 100 dedicated cancer institution in the OECI network alone along with 66 specialized cancer centres in the United Kingdom. The Royal Marsden NHS Foundation Trust still represent and forms Europe's biggest comprehensive cancer center along with The Christie NHS Foundation Trust. Our data include all cancer alliances around the Europe and United Kingdom. Through mappings we worked out that the Germany has much higher density of oncology facilities in comparison with the United Kingdom. The complete research and data are digital data for which the interested parties need a special authorisation code available on written request and one off payment.
Our research and data are collection of complete health
data covering nearly 562.7 million residents of Europe and Great Britain, includes data on individuals according to their non-cancerous
diseases, because we have also conducted a parallel review, screening an mapping of which types of patients with other diseases develop one of the cancers over time
(this is "One Off" research and data - none similar exists).