Colon / Rectum Cancer
Colorectal cancer is a disease in which cells in the colon or rectum grow out of control. Sometimes it is called colon or even bowel cancer, for short.
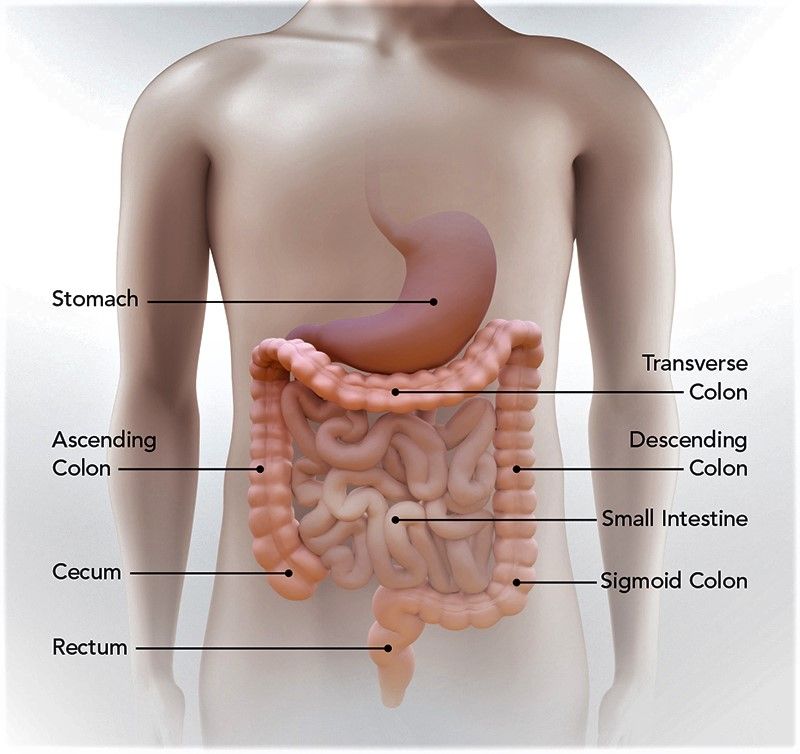
The colon is the large intestine or large bowel. The rectum is the passageway that connects the colon to the anus.
Sometimes abnormal growths, called polyps, form in the colon or rectum. Over time, some polyps may turn into cancer. Screening tests can find polyps so they can be removed before turning into cancer. Screening also helps find colorectal cancer at an early stage, when treatment works best.
Symptoms of Bowel Cancer
The 3 main symptoms of bowel cancer are:
- persistent blood in your poo – that happens for no obvious reason or is associated with a change in bowel habit
- a persistent change in your bowel habit – which is usually having to poo more and your poo may also become more runny
- persistent lower abdominal (tummy) pain, bloating or discomfort – that's always caused by eating and may be associated with loss of appetite or significant unintentional weight loss
Most people with these symptoms do not have bowel cancer. Other health problems can cause similar symptoms. For example:
- blood in the poo when associated with pain or soreness is more often caused by piles (haemorrhoids)
- a change in bowel habit or abdominal pain is usually caused by something you've eaten
- a change in bowel habit to going less often, with harder poo, is not usually caused by any serious condition – it may be worth trying laxatives before seeing a GP.
These symptoms should be taken more seriously as you get older and when they persist despite simple treatments.
When to get medical advice?
See a GP If you have any of the symptoms of bowel cancer for 3 weeks or more.
The GP may decide to:
- examine your tummy and bottom to make sure you have no lumps
- arrange for a simple blood test to check for iron deficiency anaemia – this can show whether there's any bleeding from your bowel that you have not been aware of
- arrange for you to have a simple test in hospital to make sure there's no serious cause of your symptoms
Make sure you see a GP if your symptoms persist or keep coming back after stopping treatment, regardless of their severity or your age. You'll probably be referred to hospital.
Causes of Bowel Cancer
The exact cause of bowel cancer is not known, but there are a number of things that can increase your risk, including:
- age – almost 9 in 10 people with bowel cancer are aged 60 or over
- diet – a diet high in red or processed meats and low in fibre can increase your risk
- weight – bowel cancer is more common in overweight or obese people
- exercise – being inactive increases your risk of getting bowel cancer
- alcohol – drinking alcohol might increase your risk of getting bowel cancer
- smoking – smoking may increase your chances of getting bowel cancer
- family history – having a close relative (mother or father, brother or sister) who developed bowel cancer under the age of 50 puts you at a greater lifetime risk of developing the condition; screening is offered to people in this situation, and you should discuss this with a GP
Some people also have an increased risk of bowel cancer because they've had another condition, such as extensive ulcerative colitis or Crohn's disease in the colon for more than 10 years.
Although there are some risks you cannot change, such as your age or family history, there are several ways you can lower your chances of developing the condition
COLON and RECTUM CANCER DATA Period 2020 -2025
Hospital Trials and Treatment with our NEW medications & Innovative methods
Mortality in EU 2020-2025: 985,705; (EU hospitals Standard Treatment); Our Data: 1,067,966
Mortality in the UK 2019-2024: 99,911(UK hospitals Standard Treatments); Our Data: 118,105
RESULT by OUR NEW METHODS (Used from 2014-2019) and by
OUR NEW INNOVATIVE METHODS (Used from 2020-2025+)
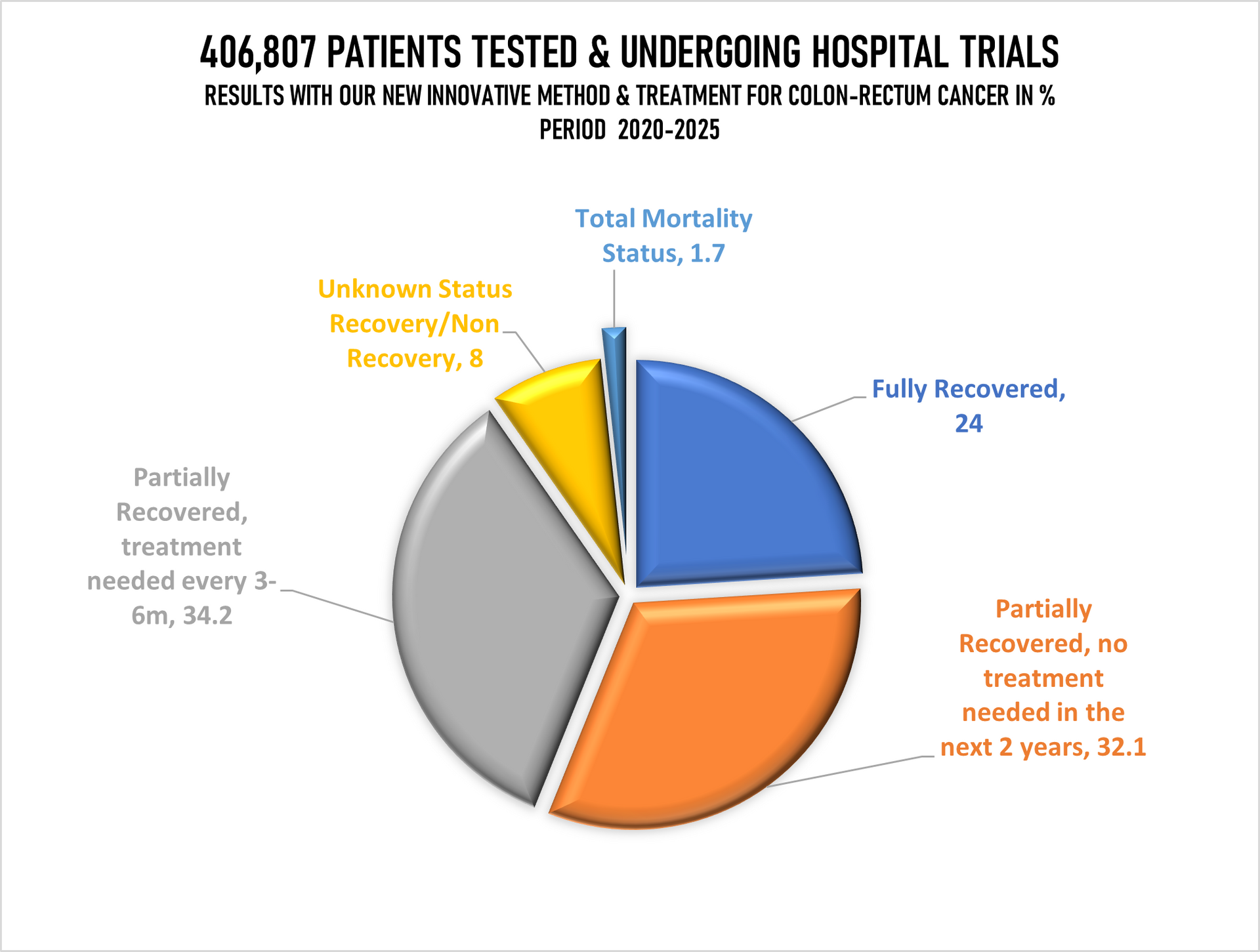
Testing Period 2020-2025; All Age Groups
Tested patients in UK, Switzerland, Germany and Italy: 406,807
Fully recovered: 24%
Recovered (No treatments needed in the next 2 years monitoring every 6 months): 32%
Partially Recovered (Further treatments needed as precaution after 3-6months passed): 34%
Unknown Recovery/ Non-recovery: 8%
Deaths in Total: Less than 2% (1.7%) (Highest % in the group 66-90).
Topics used in our core research areas along with MCCD's:
01. AI in Screening by developing AI to help find precancerous polyps more accurately during colonoscopies.
02. Focus on Immunotherapy checkpoint with ZAGEARDENAX on patients with MSI-H/dMMR tumours to the majority of patients with microsatellite-stable (MSS) tumours.
03. Metastatic Management: Improving outcomes when cancer spreads to the liver, including the study of how fatty liver disease might help cancer thrive.
04. Rectal cancer comb therapy chemo & radio - Total Neoadjuvant Therapy (TNT.
05. Research side effects like LARS (Low Anterior Resection Syndrome) and polyneuropathy caused by chemotherapy.
06. Studied specific molecular "signatures," including mutations in KRAS, NRAS, and BRAF, as well as HER2 alterations and MSI/MMR status.
07. Studying CRC rates which rising rapidly in adults under 50
08. The Gut Microbiome
09. Using blood tests to detect circulating tumour DNA (ctDNA)
REFERENCES TO THE DATA ABOVE (Period 2020-2025):
AGE GAP:
The youngest person was 11 years 10 months and 14 days of age
The oldest person was 86 years 2 month and 19 days of age
GENDER:
Female: 175,415 of 406,807
Male: 231,392 of 406,807
Age group 6-25 > 2.0%
Age group 26-45 > 22.1%
Age group 46-65 > 38.8%
Age group 66-90 > 37.1%
--------------------------------
Total: 100%
=======================
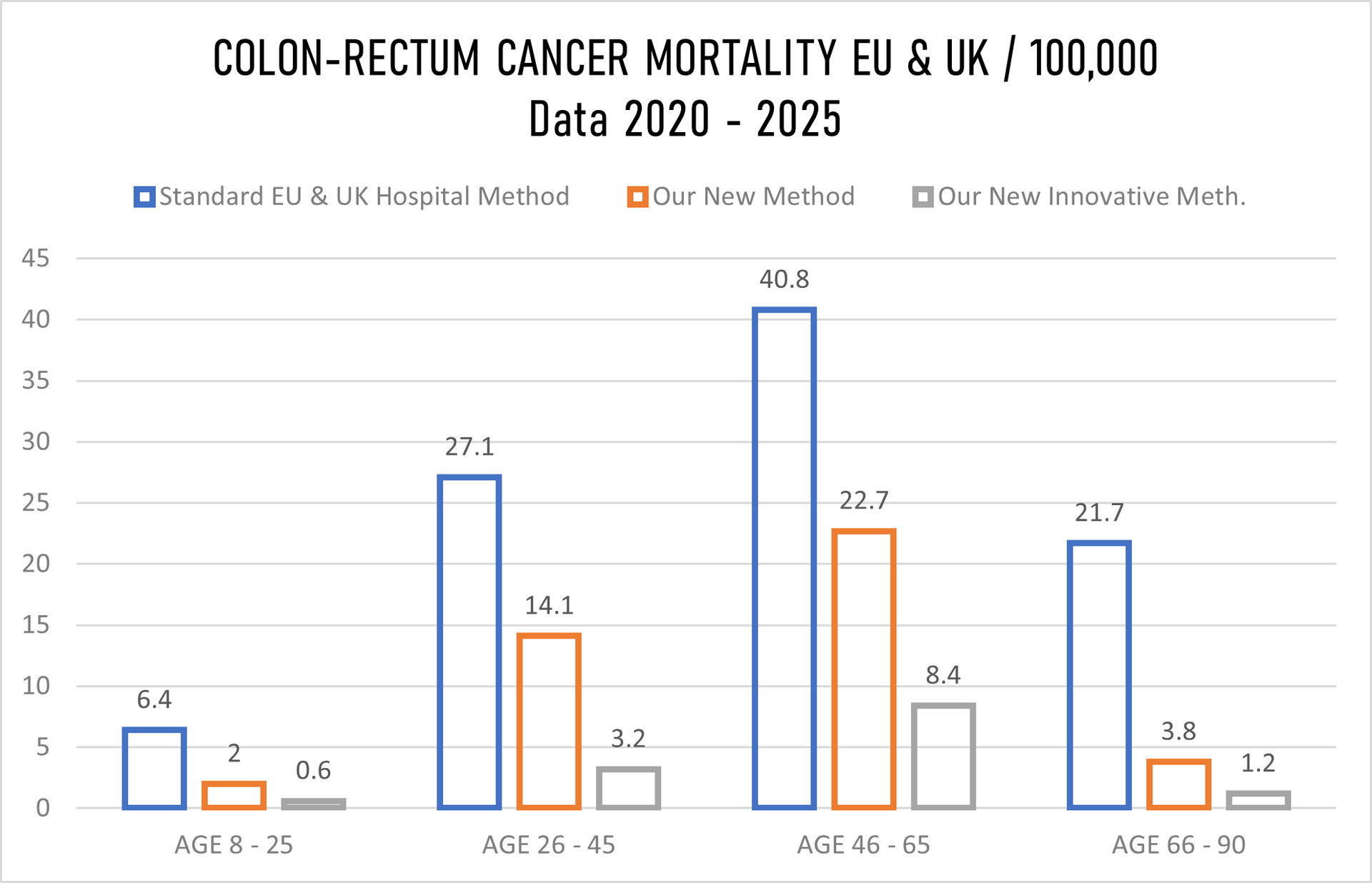
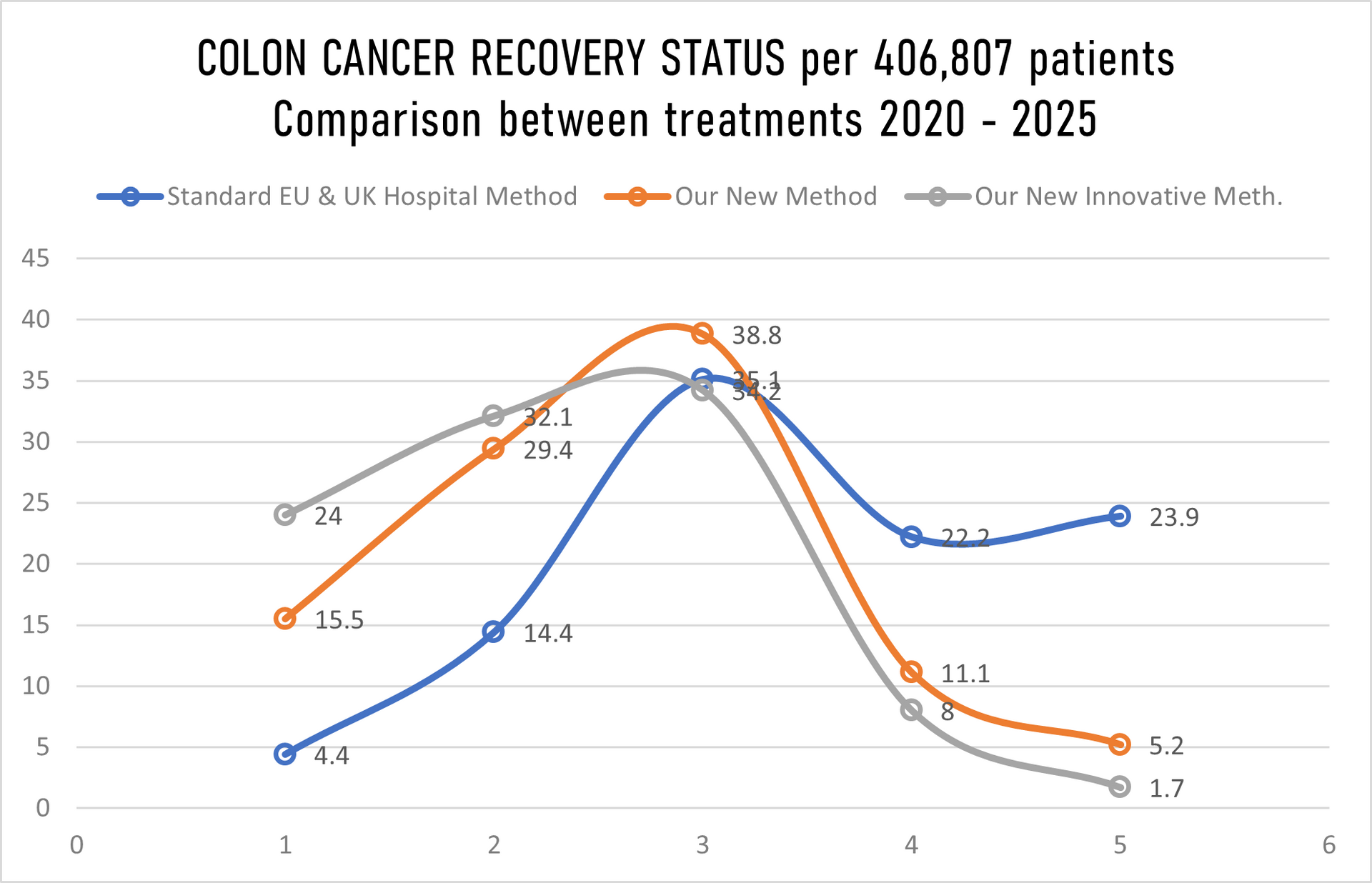
METHODS COMPARISONS:
- Old Methods meaning the STANDARD METHODS used by the general hospitals on a daily basis for the last minimum 5 years in Europe and in the United Kingdom.
- Our Methods meaning our NEW MEDICATION/TREATMENT with which we came out after over 14 years of research and tests.
- Our Innovative Methods Combine meaning our NEW INNOVATIVE MEDICATION & TREATMENT COMBINED in crossed double parallel treatment > NEW INNOVATIVE MEDICATION and different way of treatment combined with chemotherapy or combined with radiotherapy or combined with chemo and radiotherapy both together.
Separately we tested our under #2 above and #3 above combined with "OLD " methods used by the majority hospitals in Europe and in the United Kingdom however, the final readings cannot be 100 percent accurate and cannot be as such used for whatever comparison as the data across the United Kingdom and Europe are not 100 percent accurate.
MORTALITY:
In the Europe 2019-2024 > 16.3% (Going Up)
In the United Kingdom 2019-2024 > 12.9% (Going Up)
With our NEW Innovative Treatment and Medication in Europe & United Kingdom 2020-2025 less that 2% (Just 1.7%) mortality rate was recorded.
The % of "Unknown Recovery / Non-Recovery" went down to just 8% (2018/23 was 17.7%, and 2019/2024 was to 16.1% mainly in both periods at the same age group 32-44 which we believe has increased due to usage of control drugs or drugs, heavily drinking and smoking. This group is monitored separately for the third time.
There is an increase of mortality in Europe for 2.6% while in the UK mortality went up by 1.9%, yet again not hundred percent accurate data as hospitals around Europe and United Kingdom "escape" registration of the death to "push" death patient to different group as of course of the death.
All patients being chosen randomly what also might be the point of under 2% mortality rate.
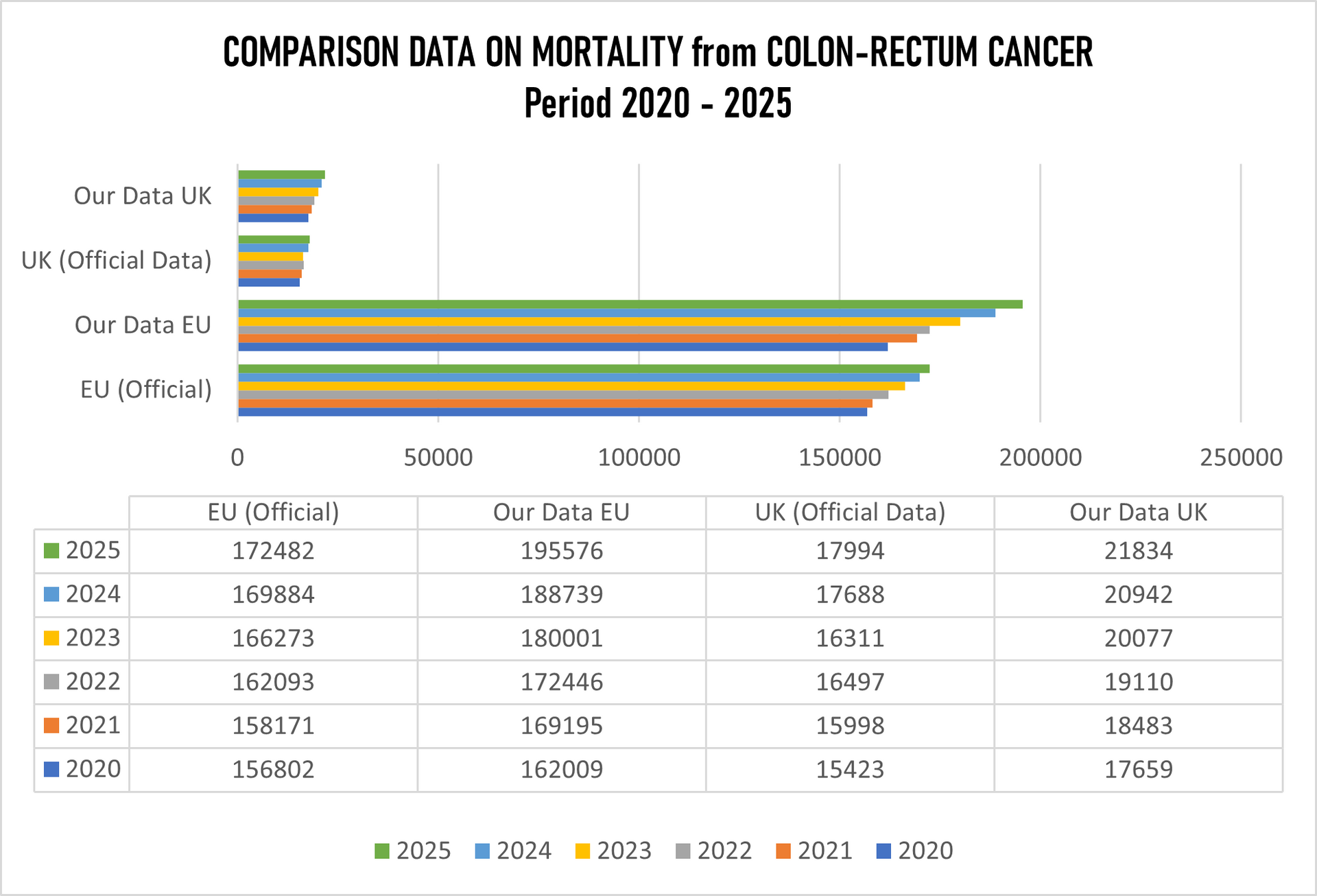
From the table above it is clearly seen that the figures are very much different. The so-called "official" data are not accurate when deaths from breast cancer are concerned, not in Europe, not in the United Kingdom. Europe claims "official" data on mortality from colon-rectum cancer is 985,705 while our data the figure is 1,067,966 which presents 82,261 deaths more.
The UK "official" data are 99,911 deaths, while our number for the same period is 118,105which is 18,194 more deaths from official data.
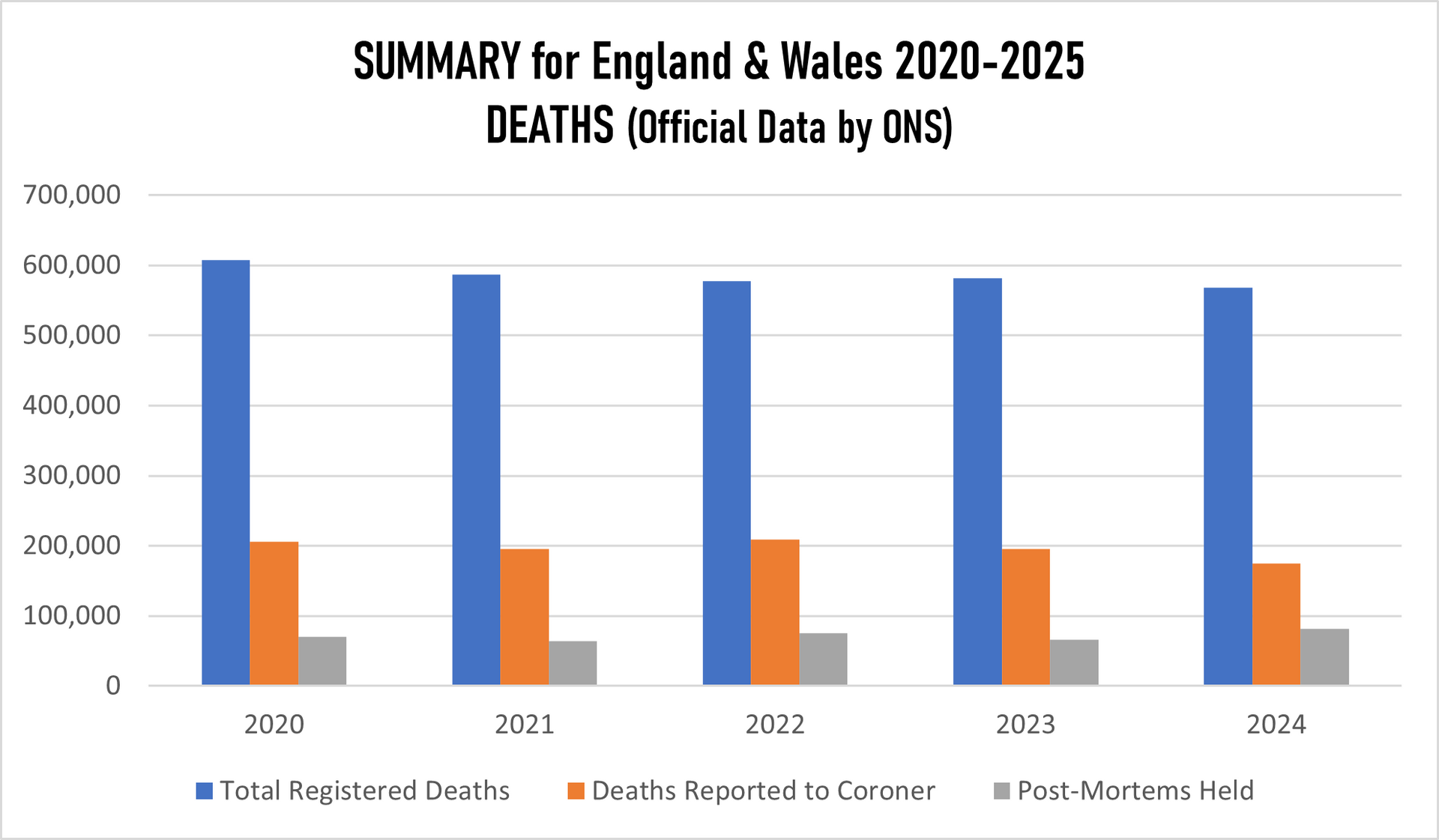
We tried to figure out how the "official" report was put together where the Office for the National Statistics is the primary source for mortality statistics in England and Wales, using data from death certificates to identify colon-rectum cancer as the underlying cause. Therefore the basics is Medical Certificate of Death (MCCD). In England in Wales the Medical Examiner Scrutiny is used (since 2024), which is statutory Medical Examiner (ME). However if the death was unexpected or sudden or the cause is unknown the coroner gets involved who might or not order a post-mortem. Yet again, the number of post-mortem examinations for colon-rectum cancer deaths is extremely low because they considered colon-rectum cancer as "natural cause" and the number of inquest and by extension has been significantly decreasing.
OUR RESEARCH and MORTALITY DATABASE 2020-2025
Cancer is one of the biggest health challenges worldwide. Since starting the research in 2011/12, the percentage of all deaths from cancer has risen from 9.6% in 2011 to 14.9% 10 years later; in the last 5 years this has risen again to where we now have 16.8% on top of the previous five years screening of all deaths recorded as cancer deaths.
Taking into consideration that in the period 2020-2025 the average European and the United Kingdom population was 762.7 million, an average 5,128,206 new cases were reported during the same period. This is an ASR of 282, and a cumulative risk of 31.28%.
Breast, Colorectum, and Lung cancers were the most common cancers across both sexes.
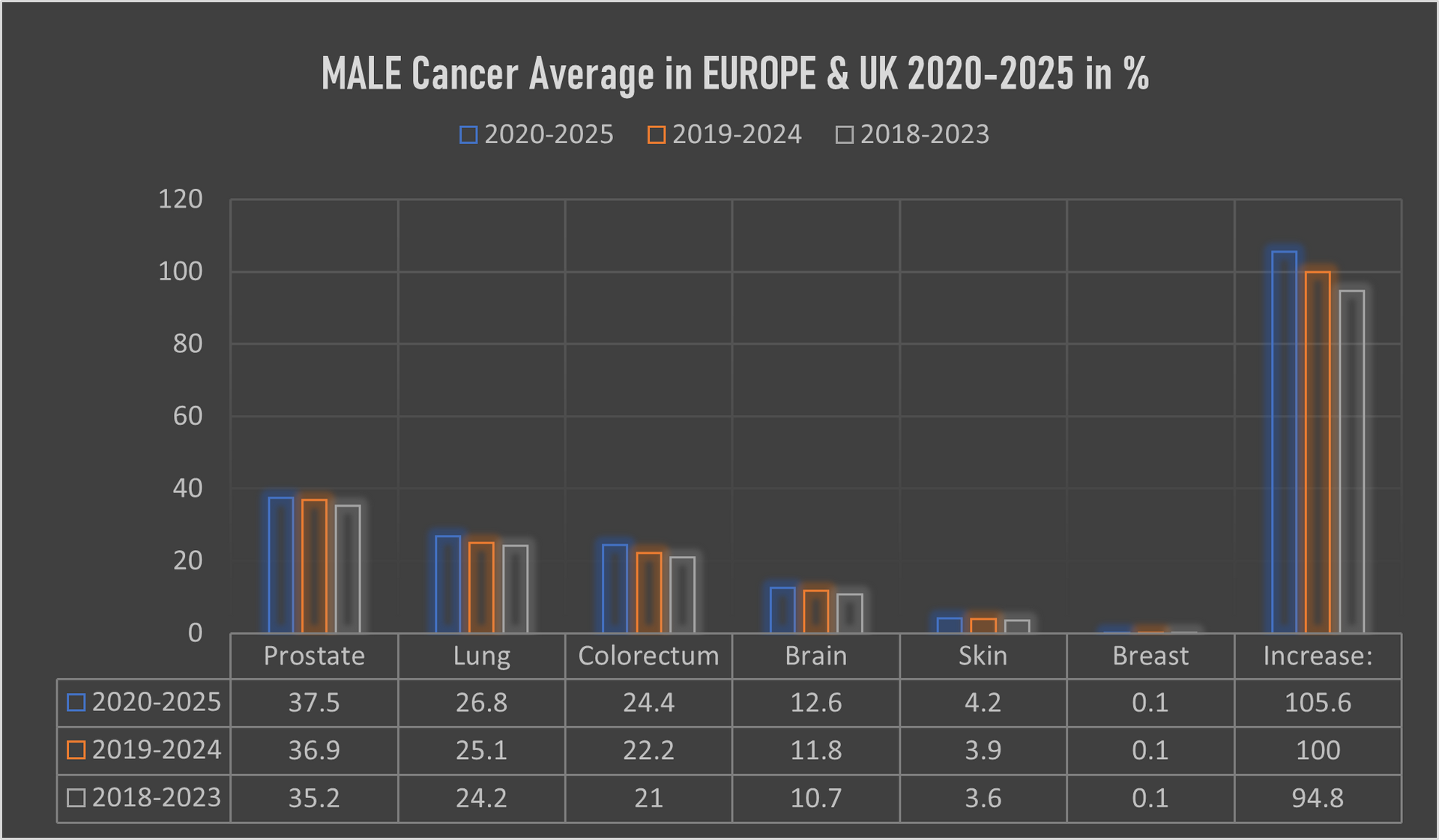
The male population in this period, some 271.4 million, recorded an average of 2,617,448 new cancer cases per year; an ASR of 327.5 per 100,000 and a cumulative risk of 34.6%.
The top 3 most common cancers among males were Prostate, Lung, and Colorectum cancer.
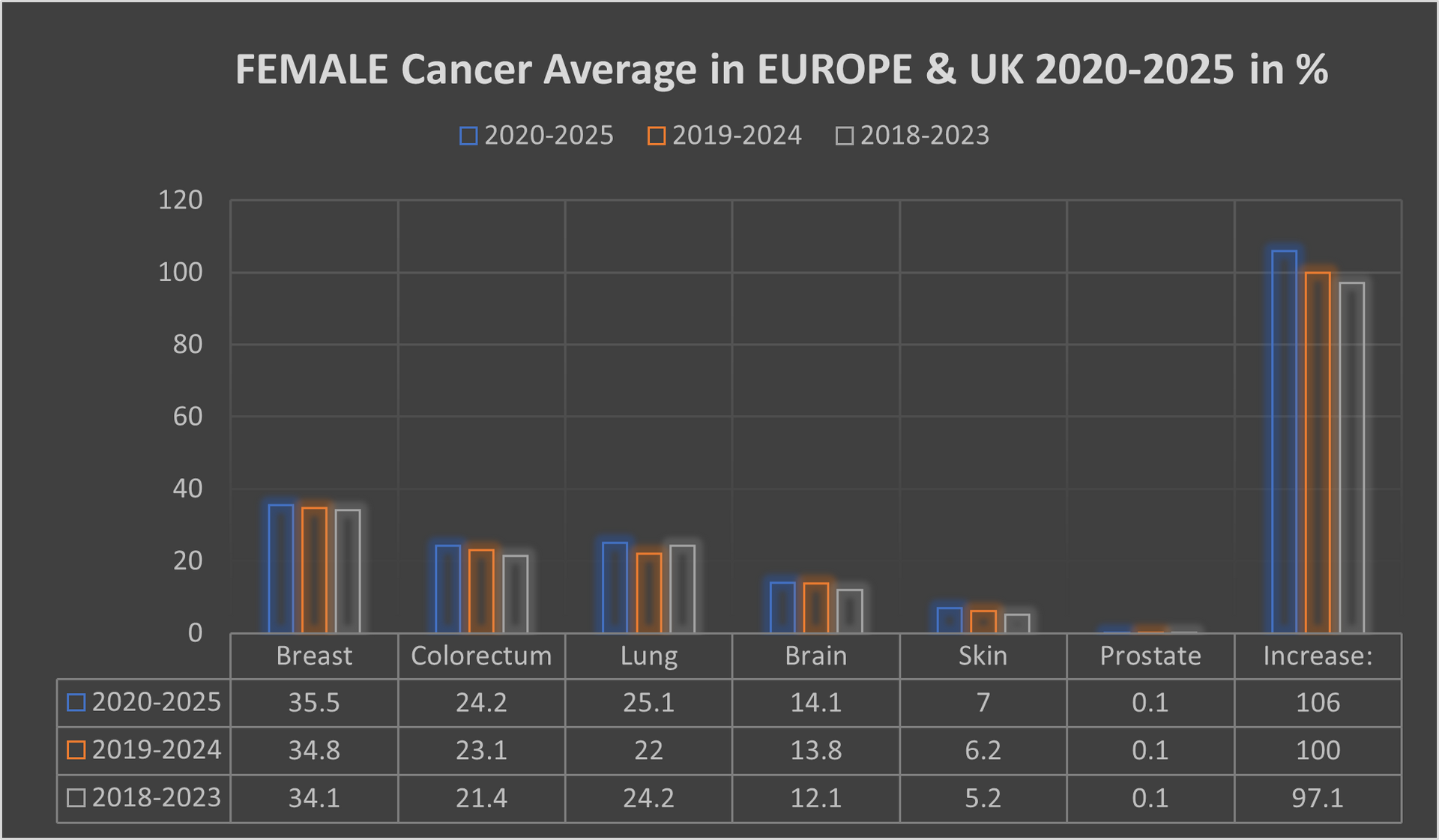
The female population in this period, some 291.3 million, recorded an average 2,494,488 new cancer cases per year; an ASR of 268.9 and a cumulative risk of 27.5%.
The top 3 most common cancers in females were Breast, Colorectum, and Lung cancer.
A significant point with cancer in the female population was switching lung cancer from 3rd place to 2nd place, with colorectum cancer dropped back from 2nd place to 3rd place.
Our mortality database is a collection of death registration data which includes cause of death information from member states; we use only the data which has been properly coded to the International Classification of Diseases (ICD).
What has also changed in recent years is the age of the death rate. This had declined over time in several countries due to life improvements, early diagnoses, medical advances, and a general reduction in risk factors like smoking and even drinking. However, there is a worrying emerging trend with rates of cancer in the population group aged up to 16.
This is rising well over expectations, especially in the United Kingdom, Spain, France and lately also in Italy.
IMPORTANT: If you are interested on details by countries, areas, hospitals we can provide all the details which include also data over 100 dedicated cancer institution in the OECI network alone along with 66 specialized cancer centres in the United Kingdom. The Royal Marsden NHS Foundation Trust still represent and forms Europe's biggest comprehensive cancer center along with The Christie NHS Foundation Trust. Our data include all cancer alliances around the Europe and United Kingdom. Through mappings we worked out that the Germany has much higher density of oncology facilities in comparison with the United Kingdom. The complete research and data are digital data for which the interested parties need a special authorisation code available on written request and one off payment.
Our research and data are collection of complete health
data covering nearly 562.7 million residents of Europe and Great Britain, includes data on individuals according to their non-cancerous
diseases, because we have also conducted a parallel review, screening an mapping of which types of patients with other diseases develop one of the cancers over time
(this is one off research - none similar exists).