Breast Cancer

Breast cancer is the most common type of cancer in the UK. Most women diagnosed with breast cancer are over the age of 50, but younger women can also get breast cancer. About 1 in 8 women are diagnosed with breast cancer during their lifetime.
There's a good chance of recovery if it's detected at an early stage. For this reason it's vital that women check their breasts regularly for any changes. In rare cases, men can also be diagnosed with breast cancer. Find out more about breast cancer in men.
Symptoms of Breast Cancer
Breast cancer can have several symptoms, but the first noticeable symptom is usually a lump or area of thickened breast tissue. Most breast lumps are not cancerous, but it's always best to have them checked by a doctor.
You should also see a GP if you notice any of these symptoms:
- a change in the size or shape of one or both breasts
- discharge from either of your nipples, which may be streaked with blood
- a lump or swelling in either of your armpits
- dimpling on the skin of your breasts
- a rash on or around your nipple
- a change in the appearance of your nipple, such as becoming sunken into your breast
- Breast pain is not usually a symptom of breast cancer.
Causes of Breast Cancer
The exact causes of breast cancer are not fully understood. However, there are certain factors known to increase the risk of breast cancer.
These include:
- age – the risk increases as you get older
- a family history of breast cancer
- a previous diagnosis of breast cancer
- a previous non-cancerous (benign) breast lump
- being tall, overweight or obese
- drinking alcohol
Diagnosing Breast Cancer
After examining your breasts, a GP may refer you to a specialist breast cancer clinic for further tests.
This might include breast screening (mammography) or taking a small sample of breast tissue to be examined under a microscope (a biopsy).

Types of Breast Cancer
There are several different types of breast cancer, which develop in different parts of the breast. Breast cancer is often divided into either:
- non-invasive breast cancer (carcinoma in situ) – found in the ducts of the breast (ductal carcinoma in situ, or DCIS) which has not spread into the breast tissue surrounding the ducts. Non-invasive breast cancer is usually found during a mammogram and rarely shows as a breast lump.
- invasive breast cancer – where the cancer cells have spread through the lining of the ducts into the surrounding breast tissue. This is the most common type of breast cancer.
Other, less common types of breast cancer include:
- invasive (and pre-invasive) lobular breast cancer
- inflammatory breast cancer
- Paget's disease of the breast
It's possible for breast cancer to spread to other parts of the body, usually through the blood or the axillary lymph nodes. These are small lymphatic glands that filter bacteria and cells from the mammary gland.
If this happens, it's known as secondary, or metastatic, breast cancer.
Breast Cancer Screening
Mammographic screening, where X-ray images of the breast are taken, is the most commonly available way of finding a change in your breast tissue (lesion) at an early stage. However, you should be aware that a mammogram might fail to detect some breast cancers.
It might also increase your chances of having extra tests and interventions, including surgery, even if you're not affected by breast cancer.
Women with a higher-than-average risk of developing breast cancer may be offered screening and genetic testing for the condition.
As the risk of breast cancer increases with age, all women who are 50 to 70 years old are invited for breast cancer screening every 3 years.
Women over the age of 70 are also entitled to screening and can arrange an appointment through their GP or local screening unit.
The National Health Service (NHS) in United Kingdom is in the process of extending the programme as a trial, offering screening to some women aged 47 to 73.
Treating Breast Cancer
If cancer is detected at an early stage, it can be treated before it spreads to other parts of the body. Breast cancer is treated using a combination of:
- surgery
- chemotherapy
- radiotherapy
Surgery is usually the first type of treatment you'll have, followed by chemotherapy or radiotherapy or, in some cases, hormone or targeted treatments.
The type of surgery and the treatment you have afterwards will depend on the type of breast cancer you have. Your doctor should discuss the best treatment plan with you.
In a small proportion of women, breast cancer is discovered after it's spread to other parts of the body (metastatic breast cancer).
Secondary cancer, also called advanced or metastatic cancer, is not curable, so the aim of treatment is to relieve symptoms.
Living with Breast Cancer
Being diagnosed with breast cancer can affect daily life in many ways, depending on what stage it's at and the treatment you will have.
How people cope with the diagnosis and treatment varies from person to person. There are several forms of support available, if you need it.
Forms of support may include:
- family and friends, who can be a powerful support system
- communicating with other people in the same situation
- finding out as much as possible about your condition
- not trying to do too much or overexerting yourself
- making time for yourself
- Find out more about living with breast cancer.
Preventing Breast Cancer
As the causes of breast cancer are not fully understood, at the moment it's not possible to know if it can be prevented. If you have an increased risk of developing the condition, some treatments are available to reduce your risk.
Studies have looked at the link between breast cancer and diet. Although there are no definite conclusions, there are benefits for women who:
- maintain a healthy weight
- exercise regularly
- have a low intake of saturated fat
- do not drink alcohol
It's been suggested that regular exercise can reduce your risk of breast cancer by almost as much as a third. Regular exercise and a healthy lifestyle can also improve the outlook for people affected by breast cancer.
If you've been through the menopause, it's particularly important that you try to get to, and maintain, a healthy weight.
This is because being overweight or obese causes more oestrogen to be produced, which can increase the risk of breast cancer
Read and find more at Breast cancer standard treatment by Zdenko Kos Foundation
Paget's disease of the Nipple

Paget's disease of the nipple, also known as Paget's disease of the breast, is a rare condition associated with breast cancer. It causes eczema-like changes to the skin of the nipple and the area of darker skin surrounding the nipple (areola). It's usually a sign of breast cancer in the tissue behind the nipple.
About 1 to 4% of women with breast cancer have Paget's disease of the nipple. It can also affect men, but this is extremely rare.
The term Paget's disease of the nipple is used to distinguish the condition from Paget's disease of the bone (where bones become weak and deformed).
BREAST CANCER DATA Period 2020 -2025
Hospital Trials and Treatment with our NEW medications & Innovative methods
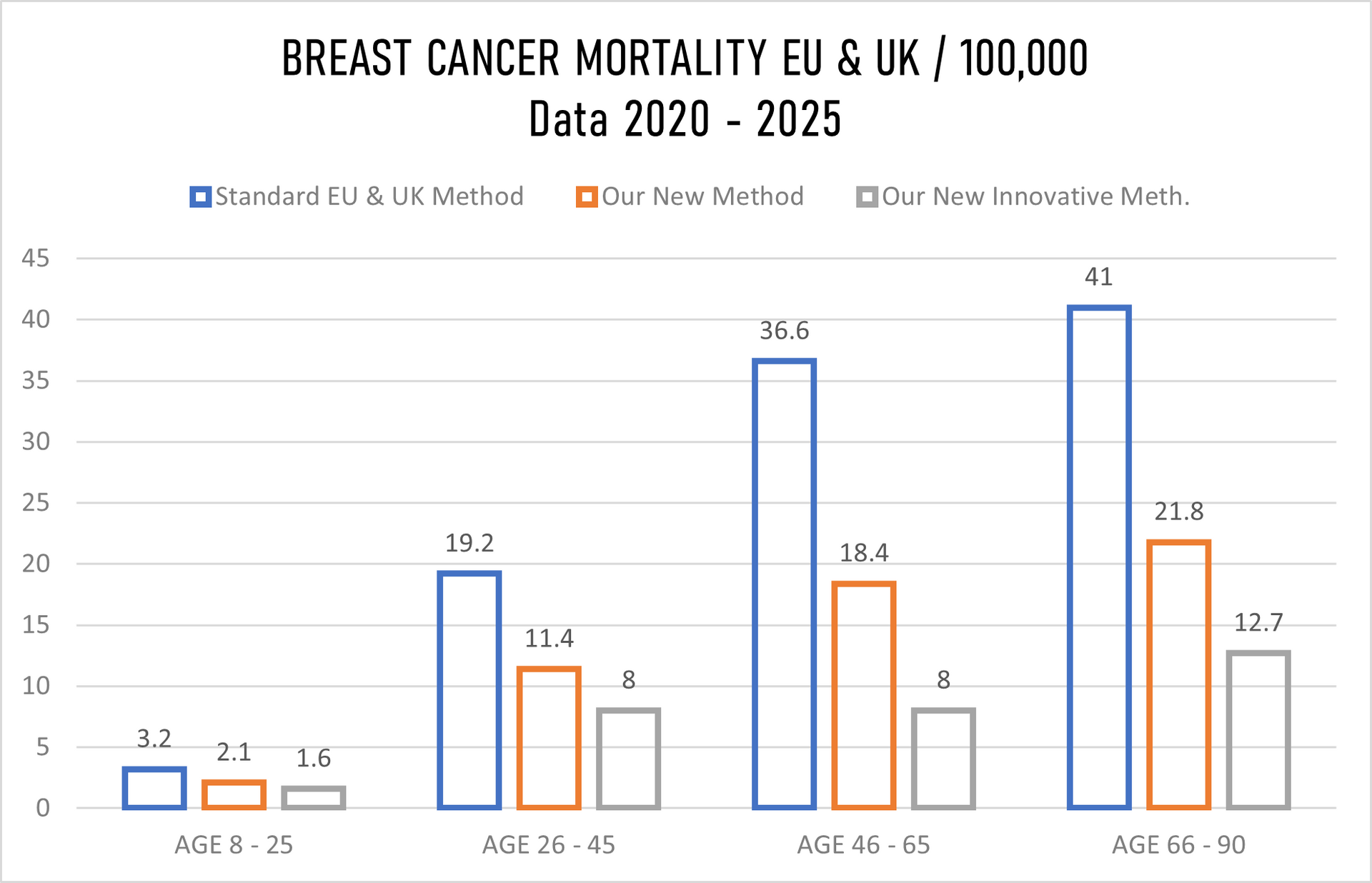
BREAST CANCER DATA Period 2020-2025
Mortality in EU 2020-2025: 811,702 (Standard EU hospitals Treatment); Our Data for EU: 866,011
Mortality in the UK 2020-2025: 73,098 (Standard UK hospital Treatment); Our Data for UK: 83,905
RESULT by OUR NEW METHODS (Used from 2014-2019) and by
OUR NEW INNOVATIVE METHODS (Used from 2020-2025+)
Testing Period 2020-2025; All Age Groups
Tested patients in the United Kingdom, Switzerland, Germany and Italy: 420,826 (100%)
Fully recovered patients: 22.4%
Recovered (No treatment needed for the period of 2 years, monitoring every 6 months: 31.8%
Partially Recovered (Further treatment needed as precautionary after 3-6 months passed): 26.2%
Unknown Recovery/Non-Recovery Data available: 15.8%
Deaths in Total: 3.8% (The highest % with the group 66-90).
Topics used in our research described along with MCCD's:
01. Artificial Intelligence (AI): Using AI-guided risk prediction
02. Comparing 3D mammography (tomosynthesis)
03. Detecting circulating tumour DNA (ctDNA)
04. Developing "smart bombs" like GARDNAMERAB Laboxtecan (registered under different name) that deliver chemotherapy directly to cancer cells while sparing healthy tissue
05. Exploring proteins like HER2 and receptors for estrogen and progesterone
06. Investigating like BRCA1 and BRCA2, PIK3CA, AKT1 - increase risk or drive progression.
07. Testing drugs like GARDNAMERAB (registered under different name) along with breast cancer vaccines
08. Using single-cell sequencing to map diverse cell populations
09. Analyze how diet, exercise, drugs, tobacco and alcohol consumption affect lifetime risk
10. Studying why some cancer cells remain inactive for years before "reawakening" to cause recurrence
11. Fertility issues for young survivors

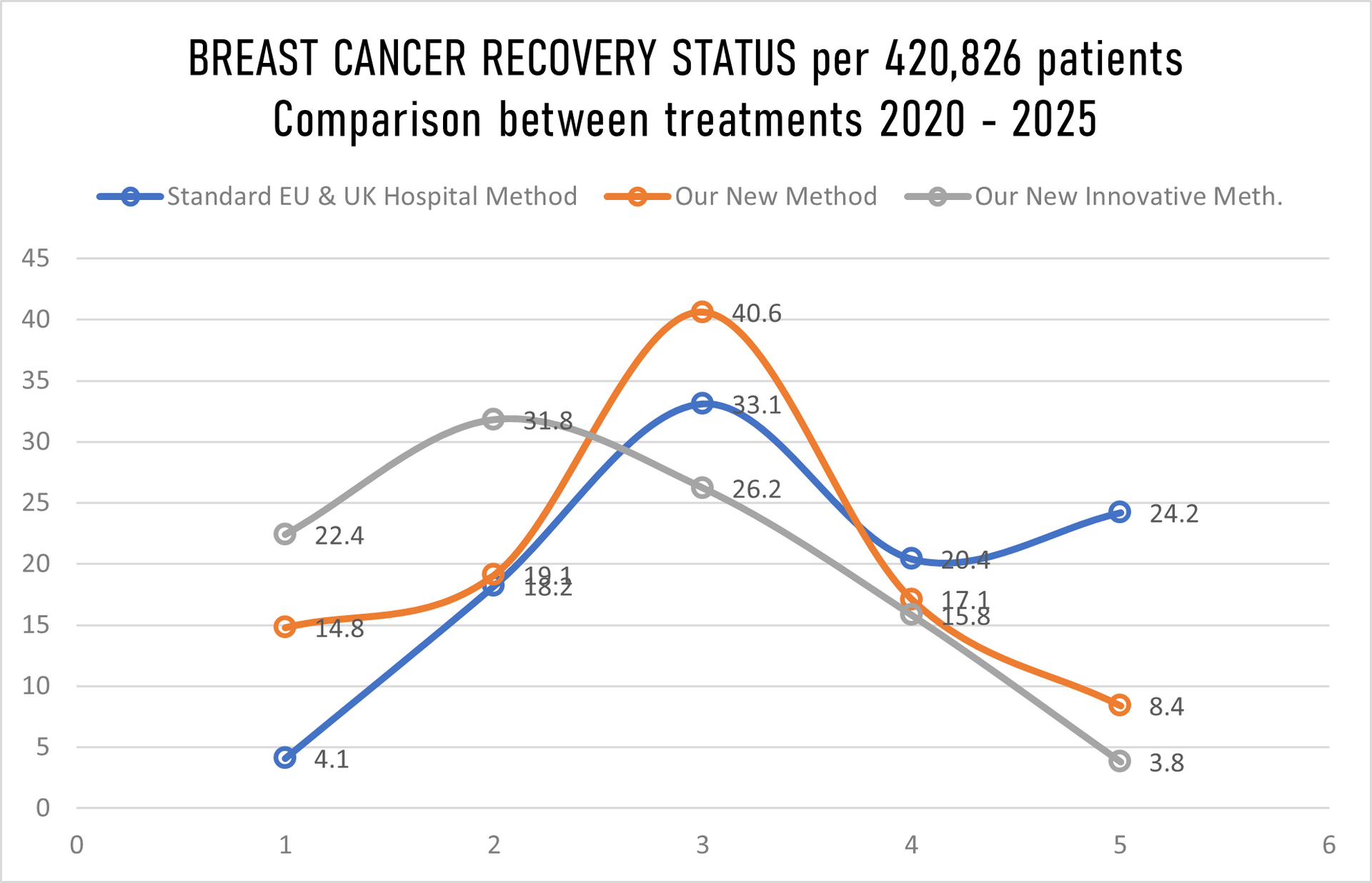
The graph above showing recovery/non-recovery status on 420,826 patients randomly taken for hospital trials and treatment where we have in
Stage 1 just 10% patients, Stage II just 20%, Stage III 30% and in Stage IV staggering 40% patients while hospitals in EU & UK gave us details for the same number of patients (420,826) in Stage 1 40%, Stage II 30%, Stage 3 20% and in Stage IV only10%. That further means that we have our mortality rate with innovative treatment well above all expectation low, sadly still 16 patients passed away despite that we overtake 40% of 580,624 patients with Stage IV cancer, in meanwhile under the standard hospital treatment in EU & UK 102 patients past away, having in mind that they have in Stage IV just 10% patients while we have 40%.
| Number of patients of 420,826 | Cancer Stage I | Cancer Stage II | Cancer Stage III | Cancer Stage IV |
|---|---|---|---|---|
| By Standard treatment in EU & UK hospital | 168,330 | 126,247 | 84,165 | 42,048 |
| By Our New Medications | 42,048 | 84,165 | 126,247 | 168,330 |
| By Our Innovative treatment | 42,048 | 84,165 | 126,247 | 168,330 |
REFERENCES TO THE DATA ABOVE (Period 2020-2025):
AGE GAP:
The youngest person was 15 years 11 months and 3 days of age
The oldest person was 88 years 4 month and 6 days of age
GENDER:
Female: 420,715 of 420,826
Male: 11 of 420,826
Age group 6-25 > 2.0%
Age group 26-45 > 22.1%
Age group 46-65 > 38.8%
Age group 66-90 > 37.1%
--------------------------------
Total: 100%
=======================
METHODS COMPARISONS:
- Old Methods meaning the STANDARD METHODS used by the general hospitals on a daily basis for the last minimum 5 years in Europe and in the United Kingdom.
- Our Methods meaning our NEW MEDICATION/TREATMENT with which we came out after over 14 years of research and tests.
- Our Innovative Methods Combine meaning our NEW INNOVATIVE MEDICATION & TREATMENT COMBINED in crossed double parallel treatment > NEW INNOVATIVE MEDICATION and different way of treatment combined with chemotherapy or combined with radiotherapy or combined with chemo and radiotherapy both together.
Separately we tested our under #2 above and #3 above combined with "OLD " methods used by the majority hospitals in Europe and in the United Kingdom however, the final readings cannot be 100 percent accurate and cannot be as such used for whatever comparison as the data across the United Kingdom and Europe are not 100 percent accurate.
MORTALITY:
In the Europe 2019-2024 > 16.3% (Going Up)
In the United Kingdom 2019-2024 > 12.9% (Going Up)
With our NEW Innovative Treatment and Medication in Europe & United Kingdom 2020-2025 less that 1% (Just 0.6%) mortality rate was recorded.
The % of "Unknown Recovery / Non-Recovery" went up (2018/23 was 15%, and 2019/2024 was to 16.1% mainly in both periods at the same age group 32-44 which we believe has increased due to usage of control drugs or drugs, heavily drinking and smoking. This group is now monitored separately for the second time.
There is an increase of mortality in Europe for 1.4% while in the UK mortality went up by 1.8%, yet again not hundred percent accurate data as hospitals around Europe and United Kingdom "escape" registration of the death to "push" death patient to different group as of course of the death.
All patients being chosen randomly what also might be the point of under 1% mortality rate.
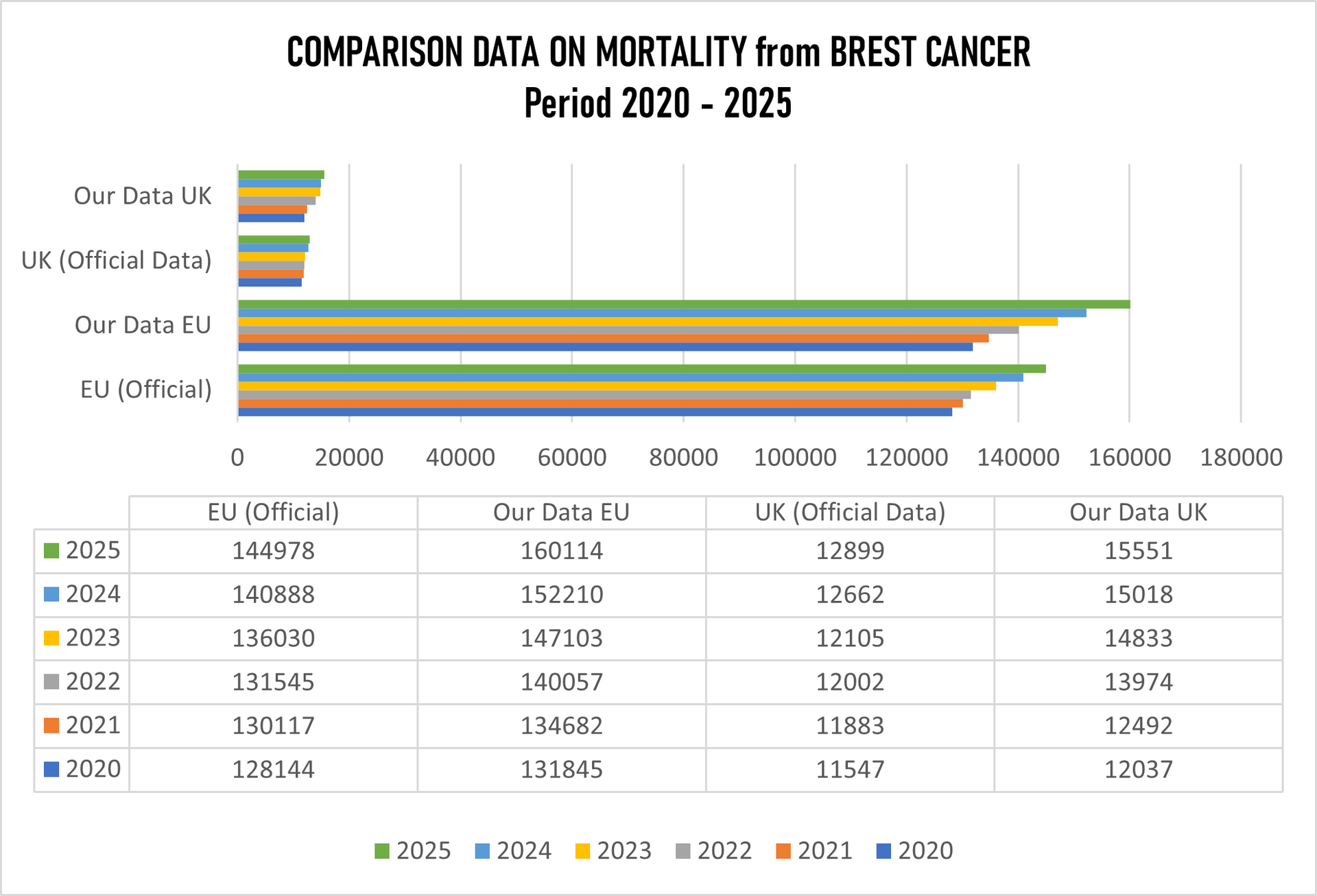
From the table above it is clearly seen that the figures are very much different. The so-called "official" data are not accurate when deaths from breast cancer are concerned, not in Europe, not in the United Kingdom. Europe claims "official" data on mortality from breast cancer is 811,702 people while our data the figure is 866,011 which presents 54,309 deaths more.
The UK "official" data are 73,098 deaths, while our number for the same period is 83,905 which is 10,807 more deaths from official data.
We tried to figure out how the "official" report was put together where the Office for the National Statistics is the primary source for mortality statistics in England and Wales, using data from death certificates to identify breast cancer as the underlying cause. Therefore the basics is Medical Certificate of Death (MCCD). In England in Wales the Medical Examiner Scrutiny is used (since 2024), which is statutory Medical Examiner (ME). However if the death was unexpected or sudden or the cause is unknown the coroner gets involved who might or not order a post-mortem. Yet again, the number of post-mortem examinations for breast cancer deaths is extremely low because they considered breast cancer as "natural cause" and the number of inquest and by extension has been significantly decreasing.
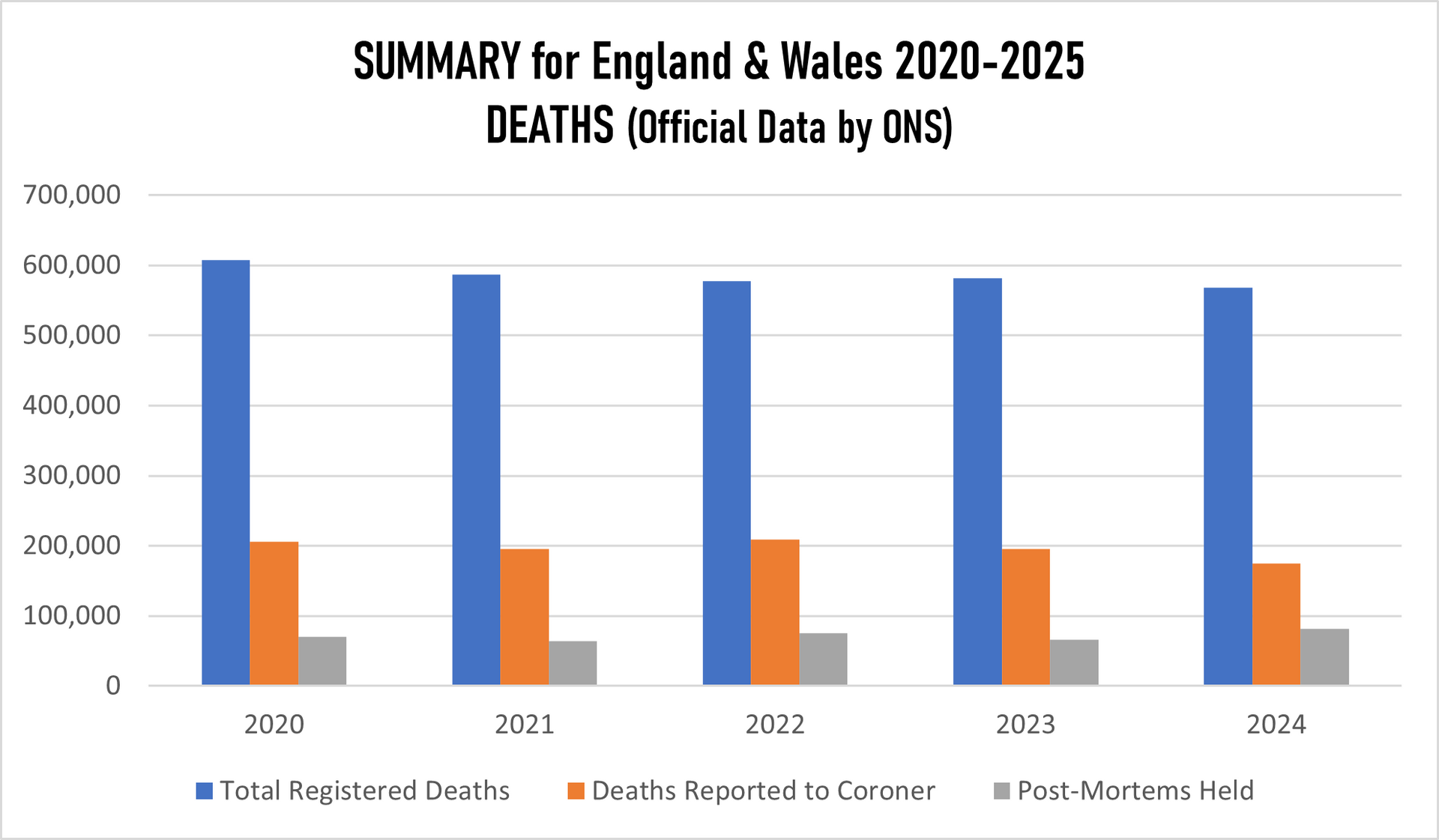
However, through our investigation it was clearly seen that there were no records of previous illnesses for the deaths considered simply because ONS and other bodies considered natural causes of death - breast cancer.
Anyway for Europe and the United Kingdom, more mammography screening programs are needed urgently, as figures are going up despite that both Europe and the United Kingdom are claiming figures are going down. Not correct at all.
OUR RESEARCH and MORTALITY DATABASE 2020-2025
Cancer is one of the biggest health challenges worldwide. Since starting the research in 2011/12, the percentage of all deaths from cancer has risen from 9.6% in 2011 to 14.9% 10 years later; in the last 5 years this has risen again to where we now have 16.8% on top of the previous five years screening of all deaths recorded as cancer deaths.
Taking into consideration that in the period 2020-2025 the average European and the United Kingdom population was 762.7 million, an average 5,128,206 new cases were reported during the same period. This is an ASR of 282, and a cumulative risk of 31.28%.
Breast, Colorectum, and Lung cancers were the most common cancers across both sexes.
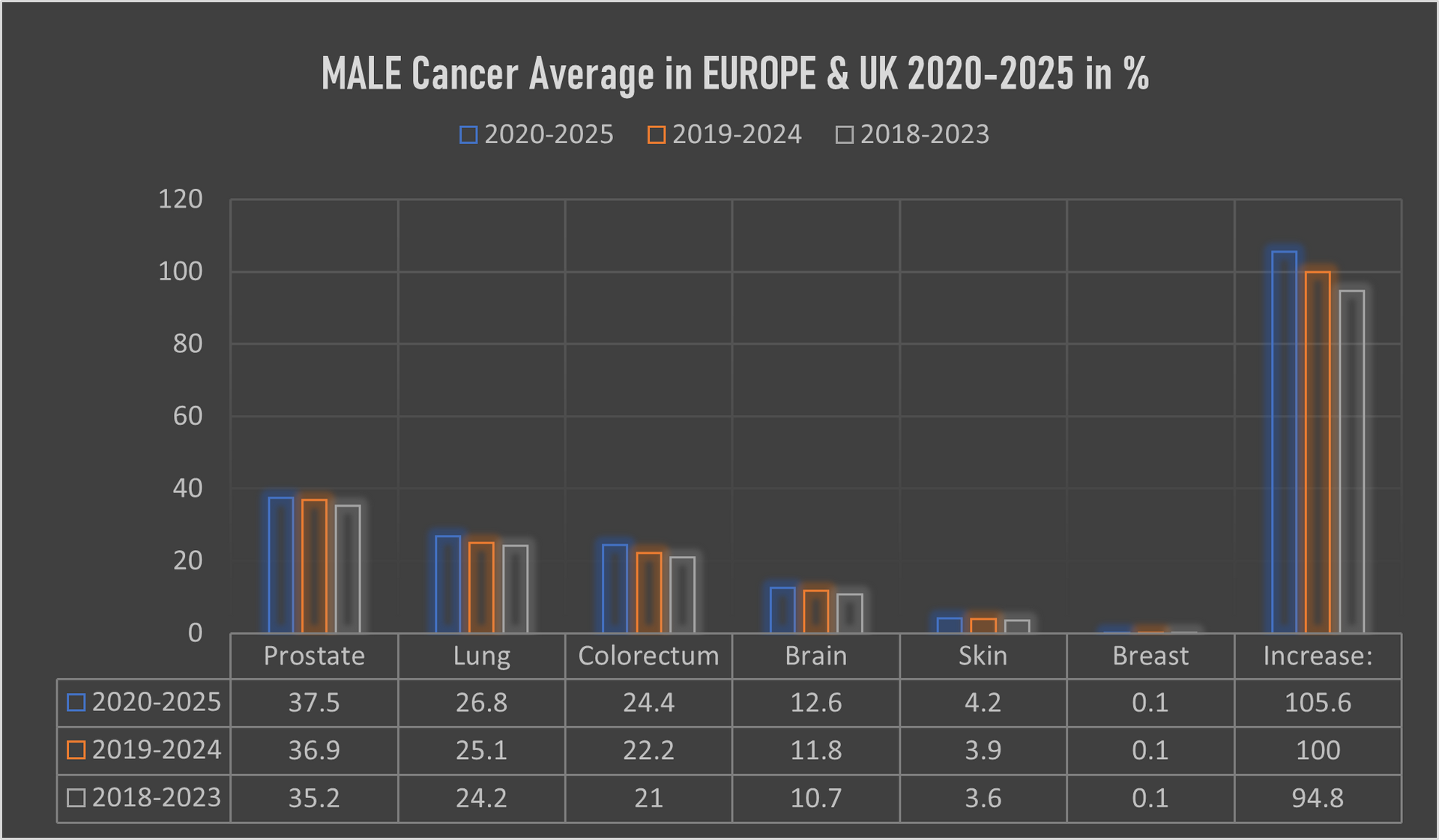
The male population in this period, some 271.4 million, recorded an average of 2,617,448 new cancer cases per year; an ASR of 327.5 per 100,000 and a cumulative risk of 34.6%.
The top 3 most common cancers among males were Prostate, Lung, and Colorectum cancer.
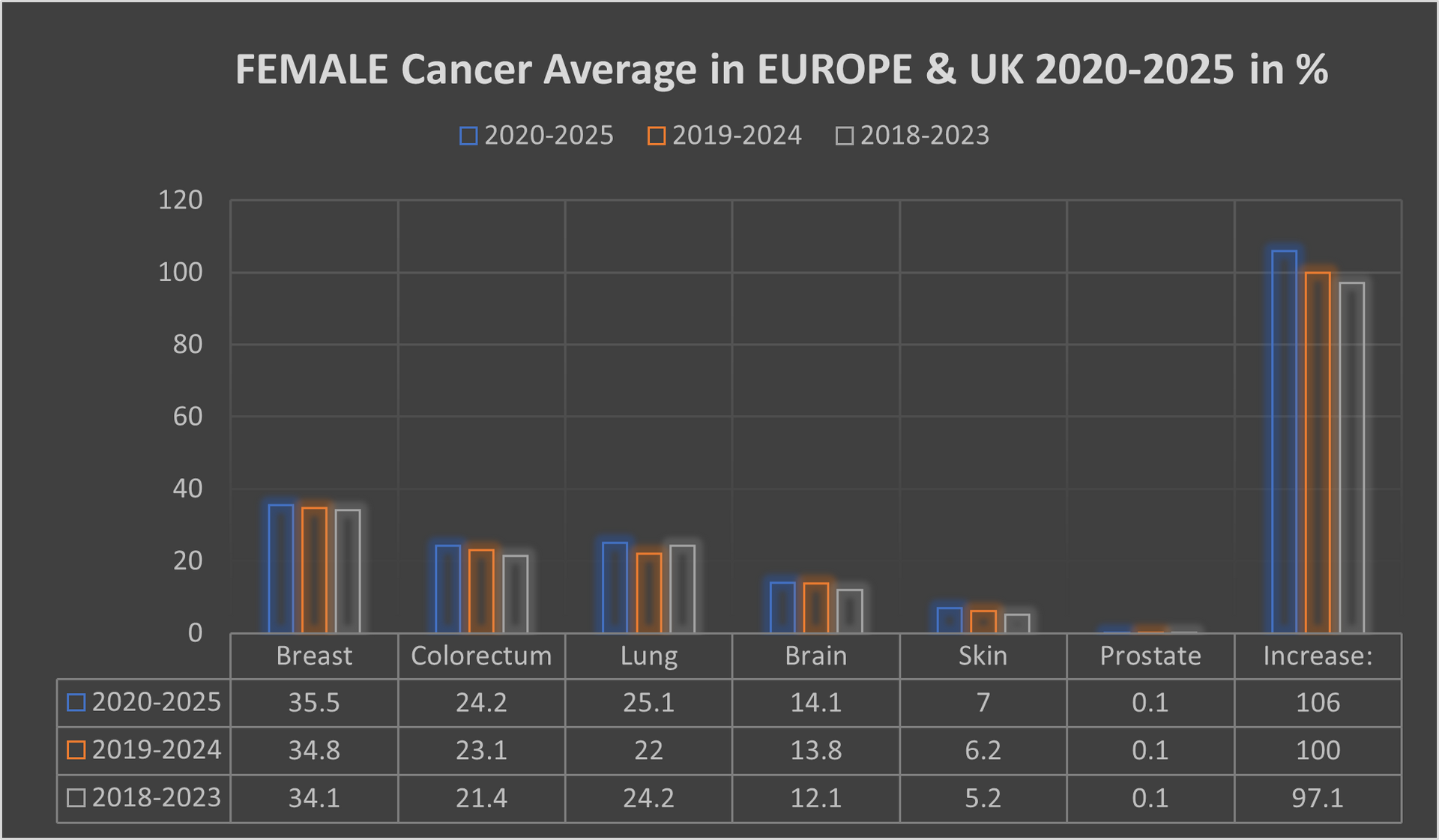
The female population in this period, some 291.3 million, recorded an average 2,494,488 new cancer cases per year; an ASR of 268.9 and a cumulative risk of 27.5%.
The top 3 most common cancers in females were Breast, Colorectum, and Lung cancer.
A significant point with cancer in the female population was switching lung cancer from 3rd place to 2nd place, with colorectum cancer dropped back from 2nd place to 3rd place.
Our mortality database is a collection of death registration data which includes cause of death information from member states; we use only the data which has been properly coded to the International Classification of Diseases (ICD).
What has also changed in recent years is the age of the death rate. This had declined over time in several countries due to life improvements, early diagnoses, medical advances, and a general reduction in risk factors like smoking and even drinking. However, there is a worrying emerging trend with rates of cancer in the population group aged up to 16.
This is rising well over expectations, especially in the United Kingdom, Spain, France and lately also in Italy.
IMPORTANT: If you are interested on details by countries, areas, hospitals we can provide all the details which include also data over 100 dedicated cancer institution in the OECI network alone along with 66 specialized cancer centres in the United Kingdom. The Royal Marsden NHS Foundation Trust still represent and forms Europe's biggest comprehensive cancer center along with The Christie NHS Foundation Trust. Our data include all cancer alliances around the Europe and United Kingdom. Through mappings we worked out that the Germany has much higher density of oncology facilities in comparison with the United Kingdom. The complete research and data are digital data for which the interested parties need a special authorisation code available on written request and one off payment.
Our research and data are collection of complete health
data covering nearly 562.7 million residents of Europe and Great Britain, includes data on individuals according to their non-cancerous
diseases, because we have also conducted a parallel review, screening an mapping of which types of patients with other diseases develop one of the cancers over time
(this is one off research - none similar exists).