Skin Cancer

There are Non-Melanoma and Melanoma Skin Cancer which is less common however usually far more serious than Non-Melanoma Skin Cancer.
There's a good chance of Non-Melanoma Skin Cancer treatment if it's detected at an early stage therefore do not hesitate to contact your GP if you have a growth on your skin that's getting bigger and bigger or has changed colour or texture.
Same applies if you have a growth or area of skin that hurts, itches, bleeds, crusts or scabs for several week.

Symptoms of Non-Melanoma Skin Cancer
The main symptom of Non-Melanoma skin cancer is a growth or unusual patch on the skin.
Any part of your skin can be affected, but it's most common in areas exposed to the sun, such as the:
- head, face and ears
- neck and shoulders
- back
- hands
- lower legs
The growths or patches can vary in colour, size and texture.
Disruption of Immune Cells in Blood
A new mole or a change in an existing mole may be signs of Melanoma.
Melanomas can appear anywhere on your body, but they're more common in areas that are often exposed to the sun.
Some rarer types can affect the eyes, soles of the feet, palms of the hands or genitals.
Check your skin for any unusual changes. Use a mirror or ask a partner or friend to check any areas you cannot see for:
- Mole with an uneven shape of edges
- Mole with a mixture of colours
- Big size - large mole's
- Mole that changes appearance over time
Symptoms of Melanoma Skin Cancer
The immune system of cancer patients are highly disrupted therefore who have a higher number of immune cells in their blood having a better survival rate.
Using special tool Immune Lymphocyte Estimation enable every researcher to calculate the proportion of T cells and B cells (types of immune cell) from whole genome sequencing (WGS) data.
WGS uses a blood sample to create a complete record of an individual's DNA.
Main causes of Non-Melanoma Skin Cancer
Ultraviolet (UV) light is the most common cause of non-melanoma skin cancer. It comes from the sun and is used in sunbeds.
Non-melanoma skin cancer is more common in older people, but younger people can also get it.
You're also more likely to get non-melanoma skin cancer if you have:
- pale skin that burns easily in the sun
- red or fair hair
- blue or green eyes
- a large number of freckles or moles
- had a lot of sun exposure and you've had sunburn a lot in the past
- used sunbeds a lot
- a history of skin cancer in your family or you've had skin cancer before
If you have brown or black skin, you have a lower chance of getting non-melanoma skin cancer, but you can still get it.
Main causes of Melanoma Skin Cancer
Melanocytes are skin cells found in the upper layer of skin. They produce a pigment known as melanin, which gives skin its colour.
There are two types of melanin:
a) Eumelanin and
b) Pheomelanin.
When skin is exposed to UV radiation from the sun or tanning beds, it causes skin damage that triggers the melanocytes to produce more melanin, but only the eumelanin pigment attempts to protect the skin by causing the skin to darken or tan.
Melanoma occurs when DNA damage from sunburns or tanning due to UV radiation triggers changes (mutations) in the melanocytes, resulting in uncontrolled cellular growth.
Lentigo Maligna
Lentigo Maligna:
This type often develops in older people. When this cancer becomes invasive or spreads beyond the original site, the disease is known as lentigo Maligna Melanoma.
This is similar to the superficial spreading type, growing close to the skin surface at first. The tumour typically arises on sun-damaged skin on the face, ears, arms or upper torso.
It may look like a flat or slightly raised, blotchy patch with uneven borders. Colour is usually blue-black, but can vary from tan to brown or dark brown.
Acral Lentiginous Melanoma
Acral lentiginous Melanoma
This is the most common type of melanoma found in people of colour including individuals of African ancestry.
It often appears in hard-to-spot places including under the nails (subungual) and on the soles of the feet or palms of the hands.
It may appear as a black or brown area on the skin.
Nodular Melanoma
Nodular Melanoma
This is the most aggressive type of melanoma. It accounts for 10 to 15 percent of all cases.
The tumour grows deeper into the skin more rapidly than other types and is most frequently found on the torso, legs and arms, as well as the scalp in older men. It is usually invasive at the time it is first diagnosed.
This type is often recognized as a bump on the skin, usually blue-black in colour, but not uncommonly can also appear as a pink to red bump.
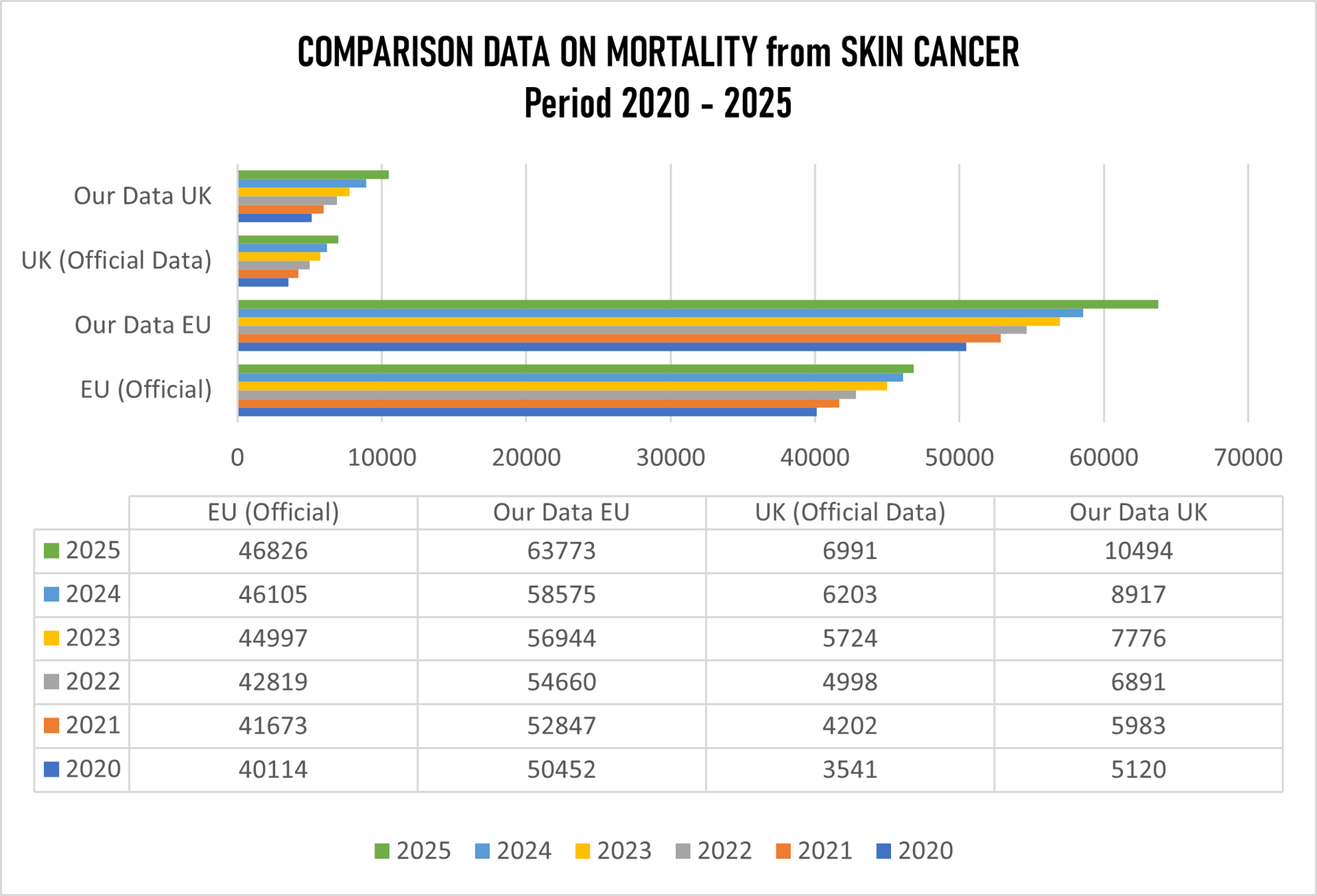
SKIN CANCER DATA Period 2020 -2025
Hospital Trials and Treatment with our NEW medications & Innovative methods
Mortality in EU 2020-2025: 1,381,522; (EU hospitals Standard Treatment); Our Data: 1,419,292
Mortality in the UK 2019-2024: 209,504 (UK hospitals Standard Treatments); Our Data: 225,089
RESULT by OUR NEW METHODS (Used from 2014-2019) and by
OUR NEW INNOVATIVE METHODS (Used from 2020-2025+)
Testing Period 2020-2025; All Age Groups
Tested patients in UK, Switzerland, Germany and Italy: 349.662
Fully recovered: 38.9%
Recovered (No treatments needed in the next 2 years monitoring every 6 months): 32.8%
Partially Recovered (Further treatments needed as precaution after 3-6months passed): 16.4%
Unknown Recovery/ Non-recovery: 11.4%
Deaths in Total: 0.5% (Highest % in the group 46-66).
Skin Cancer have 5 (five) main stages (0-IV) however with testing and hospital trials we did not consider Stage 0 (Carcinoma in Situ), where abnormal cells are found only in the top layer of the epidermis and have not invaded in tissue deeper.
Topics used in our core research areas along with MCCD's:
01. using AI and new imaging techniques to detect skin cancer earlier and examining the risks & benefits of sunlight exposure for Vitamin D.
02. Immunotherapy and Targeted Therapies: Research is developing treatments that help the immune system recognize and destroy cancer cells. Studies show that immunotherapy drugs like pembrolizumab can shrink advanced melanomas to some extend while our drugs CUTISAXADAX shrink melanomas up to 85%.
03. Identifying gene changes that cause cancer &studying how cancer cells become resistant to standard treatments like BRAF inhibitors.
04. Identifying how skin cancer spreads has identified proteins such as SLC7A11, that shield melanoma cells from environmental damage.
05. Investigating Rhenium Skin Cancer Therapy (SCT), a form of liquid radiotherapy, for non-melanoma cancers.
06. Focusing on investigating the molecule ROCK to understand how melanoma cells change shape to spread throughout the body.
07. Focusing on Drug Resistance on overcoming resistance to targeted treatments, especially for fast-growing melanomas that carry fibroblast growth factor receptor 2 mutations.
08. Focusing on CUTISAXADAX combine innovative treatment which destroyed all resistance of cancer cells without any side effects.
08. Using MARATANADAX (our drug) to improve immunotherapy using white blood cells to deliver treatments directly to tumour cells.
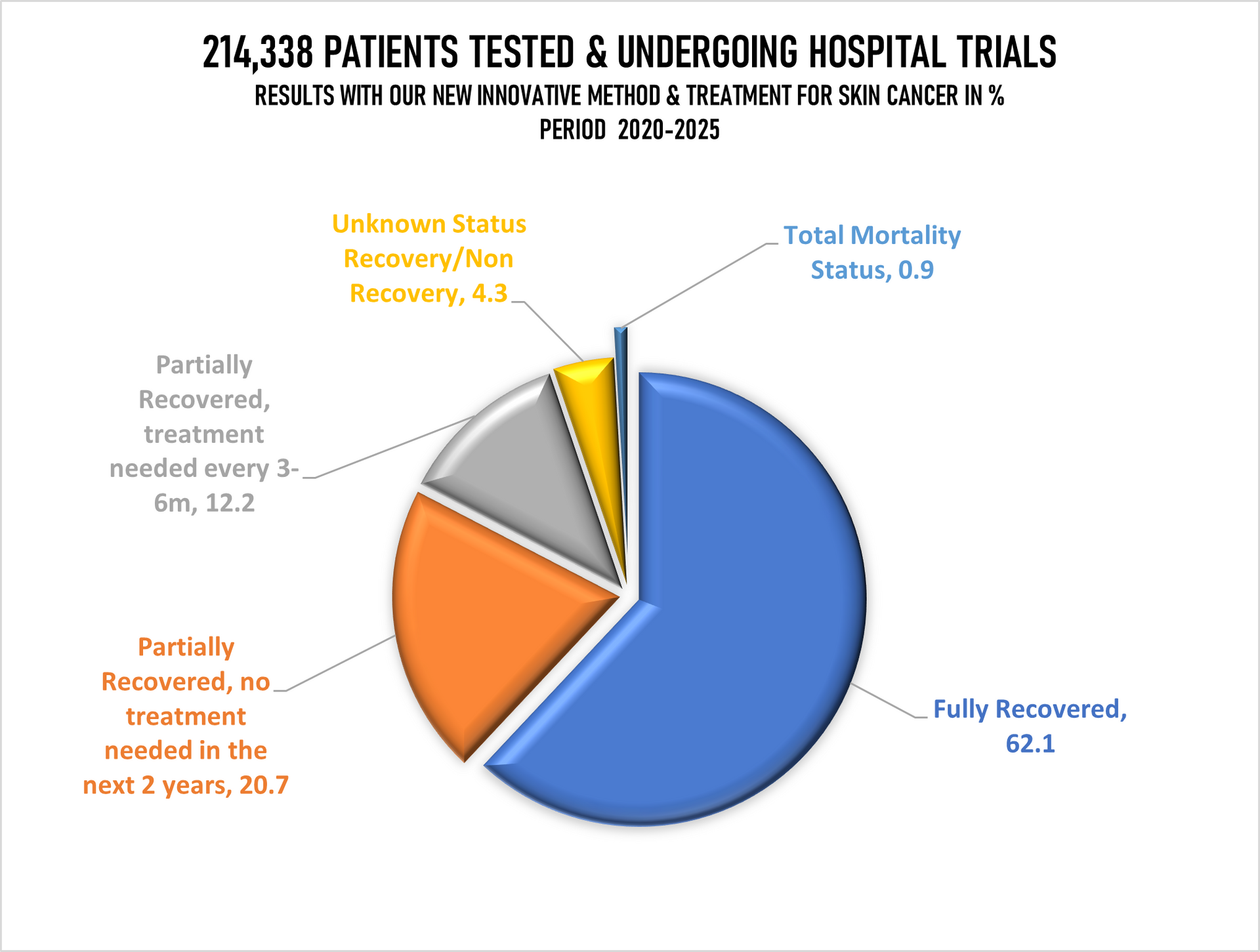
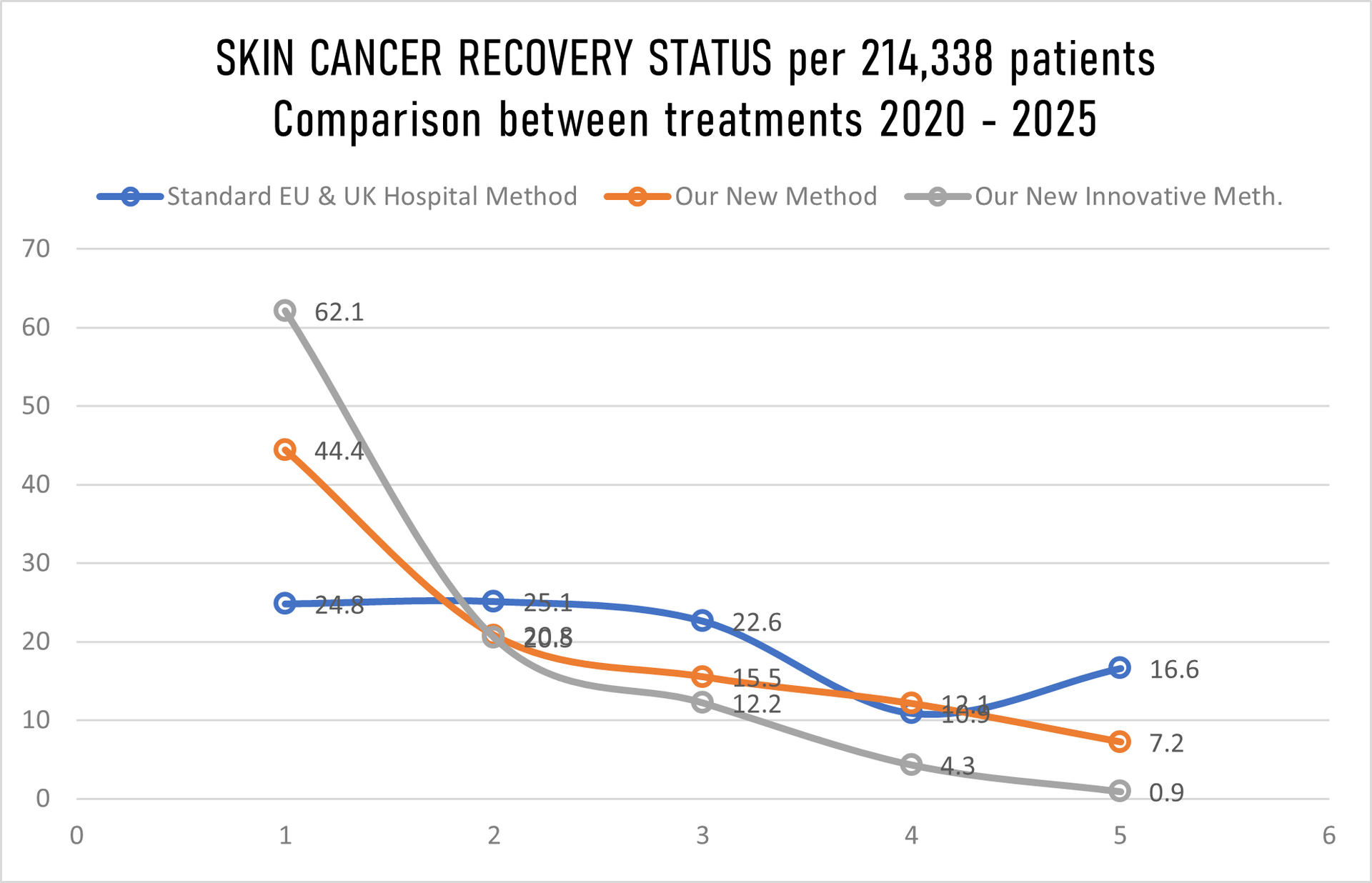
The graph above showing recovery/non-recovery status on 214,338 patients randomly taken for hospital trials and treatment where we have in
Stage 1 just 10% patients, Stage II just 20%, Stage III 30% and in Stage IV staggering 40% patients while hospitals in EU & UK gave us details for the same number of patients (214,338) in Stage 1 40%, Stage II 30%, Stage 3 20% and in Stage IV only10%. That further means that we have our mortality rate with innovative treatment well above all expectation low, sadly still 1 patients passed away despite that we overtake 40% of 214,338 patients with Stage IV cancer, in meanwhile under the standard hospital treatment in EU & UK 36 patients past away, having in mind that they have in Stage IV just 10% patients while we have 40%.
It was quite challenging to compared the data as 18 EU countries mixed data of melanoma with non-melanoma cancer. By few they were saying that patients are not passing away of Non-Melanoma Cancer. How wrong they are!
| Number of patients of 214,338 total | Cancer Stage I | Cancer Stage II | Cancer Stage III | Cancer Stage IV |
|---|---|---|---|---|
| By Standard treatment in EU & UK hospital | 85,735 | 64,301 | 42,867 | 21,435 |
| By Our New Medications | 21,435 | 42,867 | 64,301 | 85,735 |
| By Our Innovative treatment | 21,435 | 42,867 | 64,301 | 85,735 |
MORTALITY:
In the Europe 2019-2024 > 21.3% (Going Up). Most deaths in Denmark and in Slovenia.
In the United Kingdom 2019-2024 > 14.8% (Going Up)
With our NEW Innovative Treatment and Medication in Europe & United Kingdom 2020-2025 just 0.9% mortality rate was recorded.
The % of "Unknown Recovery / Non-Recovery" went down to just 4.3% (2018/23 was 17.7%, and 2019/2024 was to 18.1% mainly in both periods at the same age group 32-44 which we believe has increased due to usage of control drugs or drugs, heavily drinking and smoking and other habits. This group is monitored separately for the third time.
There is an increase of mortality in Europe for 6.7% where the cancer go up with male patients nearly for the same percentage, the most effected were Denmark, Slovenia and Slovakia, while in the UK mortality went up by 1.9%, yet again not hundred percent accurate data as hospitals around Europe and United Kingdom "escape" registration of the death to "push" death patient to different group as of course of the death.
OUR RESEARCH and MORTALITY DATABASE 2020-2025
Cancer is one of the biggest health challenges worldwide. Since starting the research in 2011/12, the percentage of all deaths from cancer has risen from 9.6% in 2011 to 14.9% 10 years later; in the last 5 years this has risen again to where we now have 16.8% on top of the previous five years screening of all deaths recorded as cancer deaths.
Taking into consideration that in the period 2020-2025 the average European and the United Kingdom population was 762.7 million, an average 5,128,206 new cases were reported during the same period. This is an ASR of 282, and a cumulative risk of 31.28%.
Breast, Colorectum, and Lung cancers were the most common cancers across both sexes.
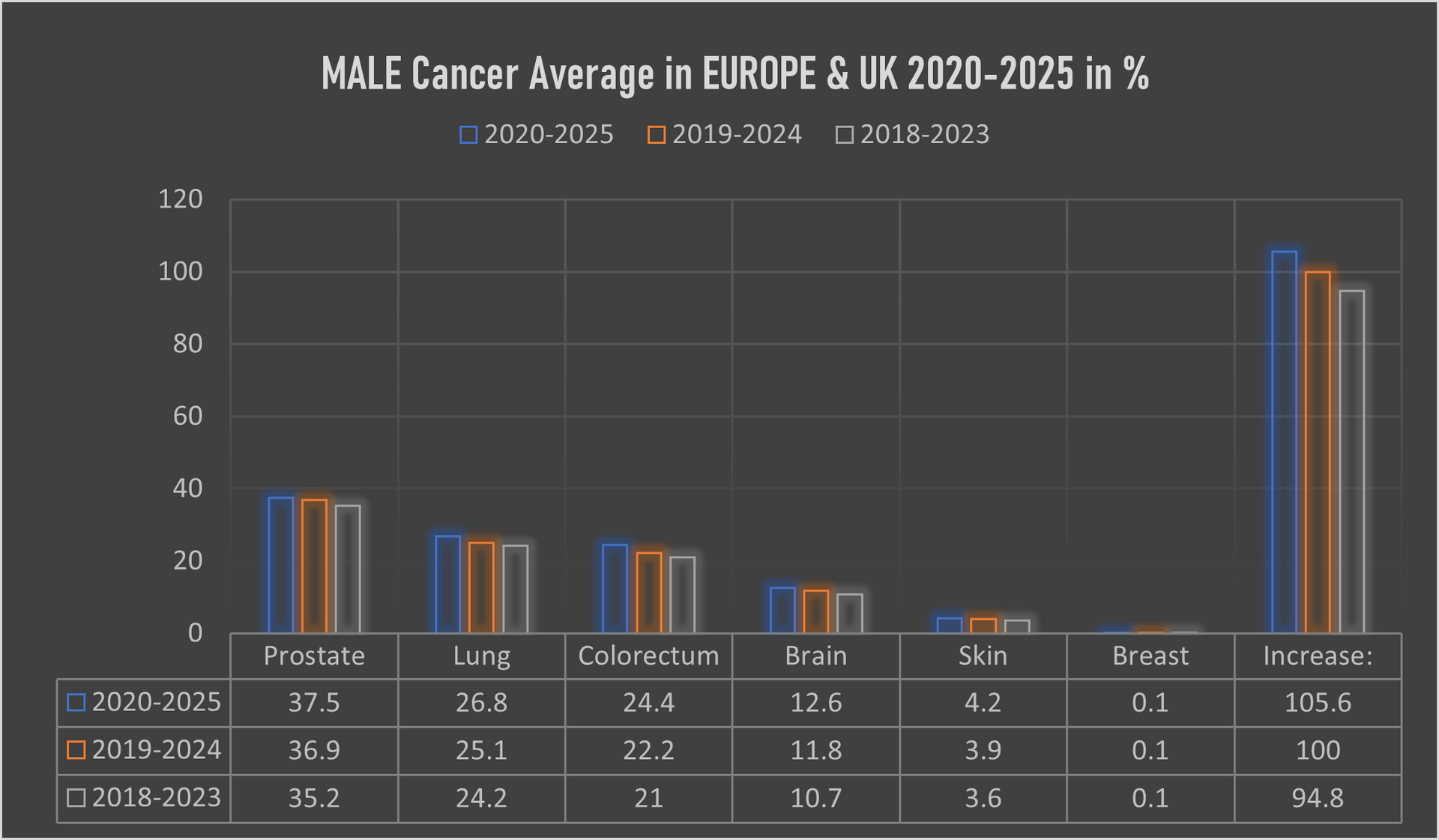
The male population in this period, some 271.4 million, recorded an average of 2,617,448 new cancer cases per year; an ASR of 327.5 per 100,000 and a cumulative risk of 34.6%.
The top 3 most common cancers among males were Prostate, Lung, and Colorectum cancer.
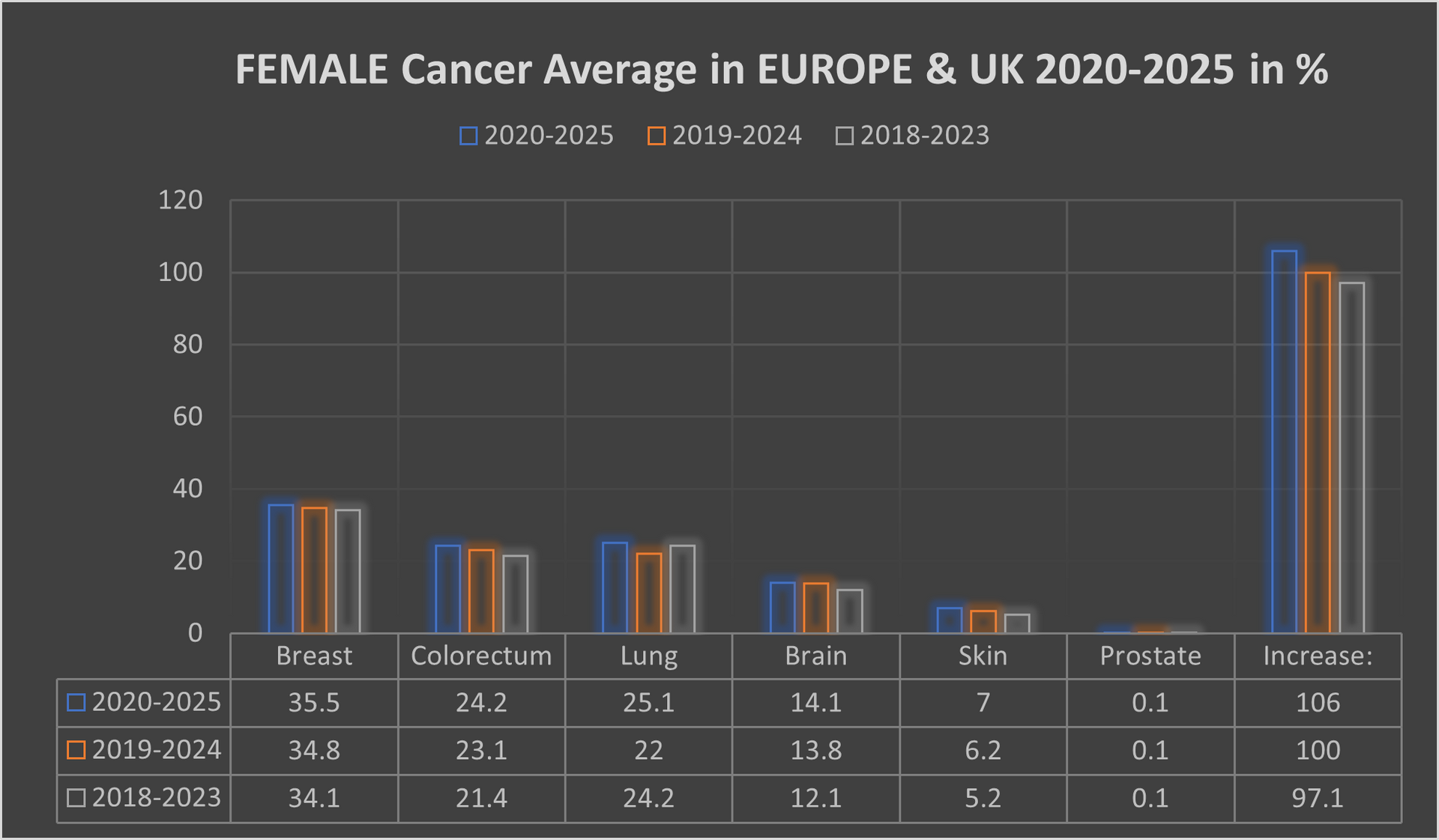
The female population in this period, some 291.3 million, recorded an average 2,494,488 new cancer cases per year; an ASR of 268.9 and a cumulative risk of 27.5%.
The top 3 most common cancers in females were Breast, Colorectum, and Lung cancer.
A significant point with cancer in the female population was switching lung cancer from 3rd place to 2nd place, with colorectum cancer dropped back from 2nd place to 3rd place.
Our mortality database is a collection of death registration data which includes cause of death information from member states; we use only the data which has been properly coded to the International Classification of Diseases (ICD).
What has also changed in recent years is the age of the death rate. This had declined over time in several countries due to life improvements, early diagnoses, medical advances, and a general reduction in risk factors like smoking and even drinking. However, there is a worrying emerging trend with rates of cancer in the population group aged up to 16.
This is rising well over expectations, especially in the United Kingdom, Spain, France and lately also in Italy.
IMPORTANT: If you are interested on details by countries, areas, hospitals we can provide all the details which include also data over 100 dedicated cancer institution in the OECI network alone along with 66 specialized cancer centres in the United Kingdom. The Royal Marsden NHS Foundation Trust still represent and forms Europe's biggest comprehensive cancer center along with The Christie NHS Foundation Trust. Our data include all cancer alliances around the Europe and United Kingdom. Through mappings we worked out that the Germany has much higher density of oncology facilities in comparison with the United Kingdom. The complete research and data are digital data for which the interested parties need a special authorisation code available on written request and one off payment.
Our research and data are collection of complete health
data covering nearly 562.7 million residents of Europe and Great Britain, includes data on individuals according to their non-cancerous
diseases, because we have also conducted a parallel review, screening an mapping of which types of patients with other diseases develop one of the cancers over time
(this is one off research - none similar exists).